As pharmacists, we play an integral role in anticipating and managing adverse events associated with conventional and novel cancer treatments. From alkylating agents to programmed cell death-1 receptor antagonists, the sheer number of agents, spectrum of toxicities, and rapidly evolving combination data make it difficult to maintain an up-to-date approach to treating patients who are at risk for adverse events.
Primary literature, abstracts, and other sources of clinical trial data such as ClinicalTrials.gov are valuable resources for clinicians to evaluate when prospectively considering side effect frequency, severity, and prevention strategies. In this issue of the Journal of Hematology Oncology Pharmacy, Joseph Bubalo, PharmD, BCPS, BCOP, provides an overview of the mechanism, prophylaxis, and evidence for the management of a common clinical question posed to pharmacists—cytarabine-induced keratoconjunctivitis (see “Prevention and Treatment of Cytarabine-Induced Keratoconjunctivitis”).
This example provides an opportunity to consider how the Common Terminology Criteria for Adverse Events (CTCAE) may be applied to daily practice. Reviewing the CTCAE reminds us that, generally, the grading of adverse events is an attempt to describe the clinical severity of a sign, symptom, or disease defined as an unintended or unfavorable event that may be associated with a procedure or medical treatment (Table).1
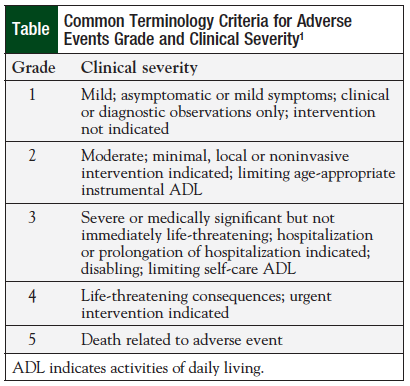
Looking at conjunctivitis as a root term in the CTCAE, it is graded from 1 to 3, with similarities to general grades listed in the Table. Specifically, grade 2 is listed as “symptomatic; topical intervention indicated (eg, antibiotics); limiting instrumental [activities of daily living].”1 Clinically, this grading suggests a patient who has clear evidence of impairment (eg, redness, pain), and who, in all likelihood, would describe this as at least bothersome if not debilitating. A key caveat to the CTCAE is that a semicolon should functionally be interpreted as “or,” meaning any one of the descriptors makes it a grade 2.
The challenge of CTCAE use has an impact on both clinical trial data reporting and interpretation. If this were a patient on a trial who was asymptomatic yet empirically given eyedrops, it automatically becomes a grade 2 toxicity based on the intervention. In clinical trial conduct, we often forget that what we do to/for patients may have an effect on toxicity grade. Similar examples and potential clinical scenarios of toxicity upgrades can be seen throughout the CTCAE in areas of importance to pharmacists, such as infusion reactions, rash, esophagitis, cytokine release syndrome, and a number of infections. Even the selection of route of administration of antibiotics can change grades, as in wound infection, where if even a single dose of intravenous antibiotics is used, the grade increases from 2 to 3 over the use of topical or oral agents.
In addition to adverse event reporting as part of clinical trials, the CTCAE may have effects on data interpretation, analysis, and translation to clinical use. Adverse events are often categorized into groups in manuscripts as “all” and “grade 3/4”; however, in many instances, clinically relevant grade 1 or 2 adverse events have direct effects on premedications, supportive care, or other aspects of patient management. With the advent of improved antiemetic agents and regimens, the definition and significance of grade 1 and 2 vomiting take on a different level of importance. If a patient receiving cisplatin has 1 to 2 episodes of vomiting in a 24-hour period after treatment, we would clinically describe that as a failure of antiemetic therapy. However, per CTCAE criteria, that is grade 1 vomiting. Similarly, grade 2 diarrhea is an increase of 4 to 6 stools daily over baseline, which, depending on other factors, most are likely to say is clinically relevant and requires intervention.
Fine-tuning CTCAE interpretation and adverse event management may require new approaches, particularly for more subjective (eg, nonlaboratory value assessments) toxicities. One area of growing research is the use of patient-reported outcomes in clinical trials. Patients consistently report more and more severe adverse events than clinicians, but end points and definitions must be carefully selected in the context of supportive care and risk–benefit ratios of anticancer treatments.2 Until these approaches are fully developed, pharmacists and other clinicians should be aware of the real and potential effects of interventions and grading in clinical trials on patient management.
References
- US Department of Health & Human Services. Common Terminology Criteria for Adverse Events (CTCAE). http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf. Updated June 14, 2010. Accessed February 25, 2015.
- Wilson MK, Collyar D, Chingos DT, et al. Outcomes and endpoints in clinical trials: bridging the divide. Lancet Oncol. 2015;16:e43-e52.