SYMPTOM OVERVIEW
Opioid-induced constipation (OIC) is a common distressing symptom in patients with cancer who are taking opioids. Although the prevalence of constipation in hospitalized patients with cancer ranges from 70% to 100%1 -with 1 study showing that the incidence of OIC in the general population is 41%2 -the occurrence of OIC in the oncology population has yet to be elucidated.
Although definitions vary, the term constipation collectively refers to the subjective impression of a decrease in the frequency of passing formed stools; difficulty and discomfort passing stools; stools of inadequate volume; or hard stools.1,3,4 Unlike other common opioid-induced side effects, minimal to no tolerance develops to OIC.3 Ongoing, untreated constipation may lead to further symptoms, including nausea and vomiting, abdominal distention, anorexia, and obstruction or fecal impaction. Thus, untreated OIC may be very distressing for the patient. Targeted pharmacologic prophylaxis and management is fundamental to the prevention or progression of opioid-induced complications.
ETIOLOGY
Opioids exert pharmacologic effects upon binding primarily to the peripheral μ-opioid receptors within the gastrointestinal (GI) mucosa.4,5 This leads to ion transport changes resulting in an inhibitory effect on neurons of the myenteric plexus, subsequently relaxing the musculature in the small intestine and colon. Multiple effects on the GI tract ensue, including delayed transit and subsequent withdrawal of water from the stool; decreased motility and tone; and decreased defecation reflexes caused by an increase in sphincter tone.1,3,5 Multiple pharmacologic options, including those aimed at reversing actions on the μ-opioid receptors in the GI mucosa, are available for prevention and treatment of OIC.
TREATMENT OPTIONS
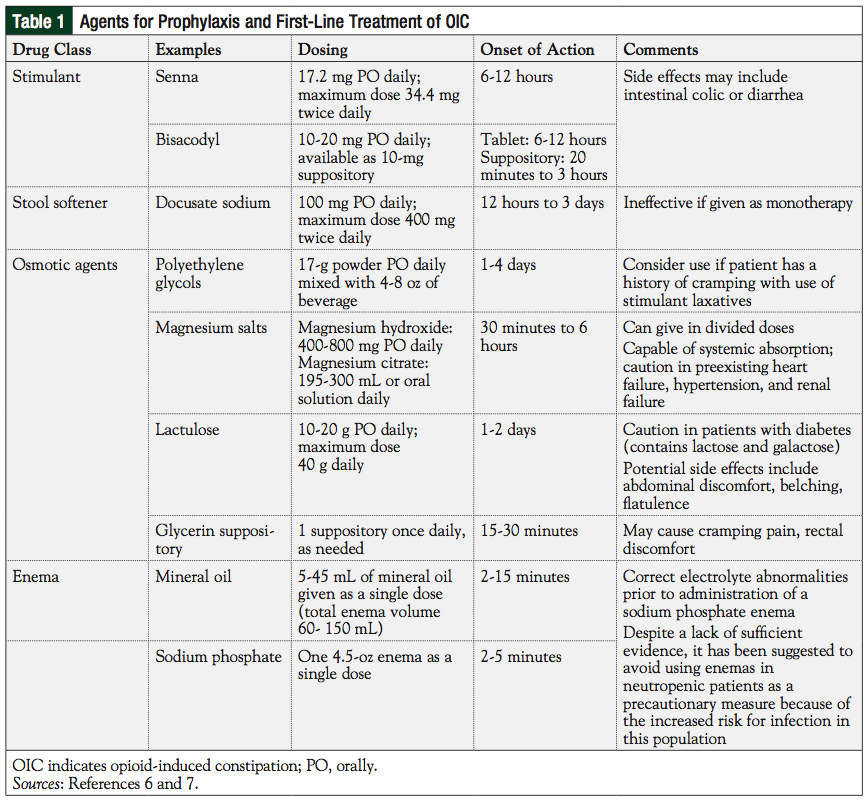
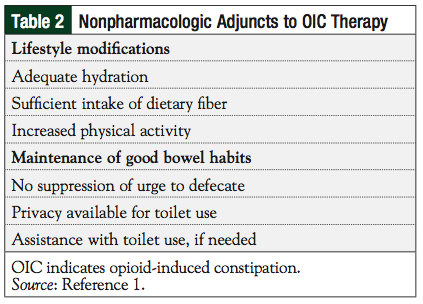
Many pharmacologic options for the management of OIC exist. The cornerstone of OIC management includes initiation of an oral standing laxative bowel regimen at the time of opioid initiation, unless contraindicated. Oral laxatives such as mineral oil, castor oil, and cascara, should not be used on a regular basis. Although laxative suppositories and enemas offer the additional benefit of stimulating the anocolonic reflex, they are not used as a prophylaxis or first-line treatment because of patient preference, potential for electrolyte disturbances, and to minimize the potential for complications that may be caused by introducing foreign bodies into the rectum.4 Typically, 1 or 2 of the agents listed in Table 16,7 are used on a scheduled basis, with supplemental dosing of an additional agent as needed, depending on bowel symptoms. Drug dosing and frequency are tailored to patient-specific needs depending on symptoms, adverse effects, cost, adherence, and contraindications. It is important to note that bulk-forming laxatives (eg, methylcellulose and psyllium) are not effective in treating OIC, and may be associated with abdominal pain and increase the risk for intestinal obstruction; thus, they are generally not recommended for OIC.3 Lifestyle modifications (Table 2), including maintaining hydration and a level of physical activity, may be helpful adjuncts to therapy, but will rarely be effective without concurrent pharmacotherapy.1 Patients should maintain good bowel habits (eg, not suppressing the urge to defecate), have adequate privacy, and receive assistance with toilet use as needed. Removal or reduction of opioid dose, if possible, may help alleviate OIC.
If initial, less expensive options fail to produce significant results after appropriate titration, then a trial with an alternative agent, such as one of the newer targeted therapies for refractory OIC (Table 3), may prove beneficial.6-10

Naloxegol (Movantik), a derivative of the μ-opioid receptor antagonist naloxone, is indicated for the treatment of OIC in patients with noncancer pain.8 Its pegylated chemical structure prohibits it from crossing the blood-brain barrier, and it maintains a solely peripheral mechanism of action. Two identical, phase 3, clinical, placebo-controlled trials of naloxegol were conducted in adult patients using stable regimens of opioids for noncancer pain.11 Patients were randomly assigned in a 1:1:1 ratio to receive an oral daily dose of 12.5 mg or 25 mg of naloxegol, or placebo for 12 weeks. Response rates were defined as ≥3 unplanned bowel movements each week, and an increase from baseline of ≥1 spontaneous bowel movements for ≥9 of the 12 weeks, and ≥3 of the 4 final weeks. In both studies, patients taking 25 mg of naloxegol showed a significantly greater response rate during 12 weeks compared with placebo (P = .001 and P = .02, respectively). In one study, patients taking 12.5 mg also demonstrated significant improvement compared with placebo (P = .02). Other end points, such as time to the first spontaneous bowel movement, severity of straining, and stool consistency, were better for patients using naloxegol compared with placebo. The most commonly reported adverse events were GI in nature (ie, diarrhea, nausea, vomiting, abdominal pain) and more common in the group taking 25 mg. It is recommended to discontinue other laxatives when starting naloxegol.8 However, other laxatives may be restarted if the patient does not produce a bowel movement within 72 hours after starting naloxegol.
Methylnaltrexone bromide (Relistor) is a peripherally acting μ-opioid receptor antagonist that is US Food and Drug Administration (FDA) approved for the treatment of OIC in patients with advanced illness who are receiving palliative care, when response to laxative treatment has not been sufficient.9 It is administered via subcutaneous injection in the upper arm, abdomen, or thigh, every other day as needed. In a randomized, double-blind, placebo-controlled study, 133 patients who used opioids for ≥2 weeks, were at stable doses, and used laxatives for ≥3 days without relief, were randomized to receive 0.15 mg/kg of methylnaltrexone subcutaneously every other day, or placebo, for 2 weeks.12 Forty-eight percent of patients in the methylnaltrexone group had laxation within 4 hours of receiving the first dose compared with 15% in the placebo group (P <.001). The average time to laxation after the first dose was 6.3 hours in the methylnaltrexone group versus >48 hours for patients receiving placebo (P <.001). There was no evidence of opioid receptor withdrawal symptoms during the study. Adverse reactions of abdominal pain, flatulence, nausea, increased body temperature, and dizziness were more prevalent in the methylnaltrexone group. All serious reactions (eg, progression of malignant neoplasm) were determined unlikely to have been related to the study drug.
Lubiprostone (Amitiza) is a locally acting chloride channel activator, previously indicated only for the treatment of idiopathic constipation and irritable bowel syndrome with constipation in women aged ≥18 years.10 In 2013, it gained FDA approval for OIC.13 This medication increases intestinal fluid secretion without altering serum sodium or potassium levels. The increased fluid secretion in the intestines serves to improve intestinal motility, allowing easier passage of stool. A randomized, double-blind, placebo-controlled study of 418 patients using stable doses of opioid for chronic noncancer pain found that oral lubiprostone 24 μg twice daily was significantly better than placebo at improving the occurrence of spontaneous bowel movements (3.3 vs 2.4 per week at 8 weeks; P = .005).13 Compared with placebo, more patients who received lubiprostone had their first spontaneous bowel movement within 24 hours (P = .018) and 48 hours (P = .050) of receiving their first dose of the study medication. Patients in the lubiprostone group reported significant improvements in symptoms of abdominal discomfort, straining, constipation severity, and stool consistency, compared with placebo. Nausea, diarrhea, and abdominal distention were the most frequently reported adverse events, occurring more commonly in the lubiprostone group.
OIC is a frequent problem encountered in patients with cancer. In cases where removal of the offending agent is not possible because of the need for analgesia, aggressive prophylactic measures should be taken, with a regimen developed and tailored to patient-specific needs depending on symptoms, adverse effects, cost, compliance, and contraindications. In the case of refractory OIC, one of the more novel agents may prove beneficial to avoid further escalation of distressing symptoms and life-threatening complications. As additional targeted drugs are developed, and further evidence from larger, high-quality trials becomes available, clinicians should expect to see development of a more standardized approach to treating and preventing constipation.
Author Disclosure Statement
Dr Winans and Dr Sera reported no conflicts of interest. Dr Pawasauskas is on the Speakers' Bureau for Mallinckrodt Pharmaceuticals.
References
1. McMillan SC. Assessing and managing opiate-induced constipation in adults with cancer. Cancer Control. 2004;11(Suppl 3):3-9.
2. Kalso E, Edwards JE, Moore A, et al. Opioids in chronic non-cancer pain: systematic review of efficacy and safety. Pain. 2004;112:372-380.
3. Clemens KE, Klaschik E. Management of constipation in palliative care patients. Curr Opin Support Palliat Care. 2008;2:22-27.
4. Wein S. Opioid-induced constipation. J Pain Palliat Care Pharmacother. 2012;26:382-384.
5. Camilleri M. Opioid-induced constipation: challenges and therapeutic opportunities. Am J Gastroenterol. 2011;106:835-842.
6. Lexi-Comp, Inc (Lexi-Drugs®). Lexi-Comp, Inc; March 3, 2015.
7. Twycross R, Sykes N, Mihalyo M, et al. Stimulant laxatives and opioid-induced constipation. J Pain Symptom Manage. 2012;43:306-313.
8. Movantik [package insert]. Wilmington, DE: AstraZeneca; 2015.
9. Relistor [package insert]. Raleigh, NC: Salix Pharmaceuticals, Inc; 2014.
10. Amitiza [package insert]. Bethesda, MD: Sucampo Pharmaceuticals, Inc; 2013.
11. Chey WD, Lebster L, Sostek M, et al. Naloxegol for opioid-induced constipation in patients with noncancer pain. N Engl J Med. 2014;370:2387-2396.
12. Thomas J, Karver S, Cooney GA, et al. Methylnaltrexone for opioid-induced constipation in advanced illness. N Engl J Med. 2008;358:2332-2343.
13. Cryer B, Katz S, Vallejo R, et al. A randomized study of lubiprostone for opioid-induced constipation in patients with chronic noncancer pain. Pain Med. 2014;15:1825-1834.

