Symptom Overview
Corneal toxicity with high-dose cytarabine is a well-established risk of therapy.1 Routine prophylaxis with eye drops, usually topical corticosteroid drops, is an established part of high-dose cytarabine treatment protocols.2 Without topical corticosteroid prophylaxis, incidences of keratoconjunctivitis have been reported in 85% to 100% of cases3,4; the occurrence of clinically significant symptoms with the use of prophylaxis is reported in 8% to 16% of cases.3
Etiology
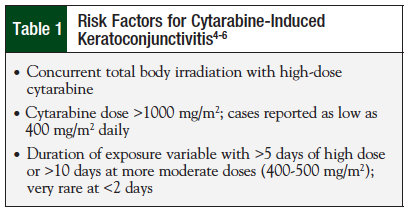
Cytarabine has a known ability to penetrate body fluids, including crossing the blood–brain barrier, and can be found in the aqueous humor and in tears.5 Corneal toxicity appears to be related to the concentration of cytarabine in tears, and the duration of exposure. Risk factors vary with high-dose cytarabine (Table 1), and duration of dosing is most strongly associated with the toxicity4-6; few cases have been seen with intermittent or continuously administered intravenous, low-dose cytarabine (eg, <200 mg/m2/day).5 Conjunctivitis has occurred as early as 3 days into therapy, and several days after therapy, with days 6 to 8 posttherapy the most commonly reported time of occurrence.6-8
Findings at eye examinations have been described as bilateral corneal epithelial microcysts—possibly more densely distributed in the center of the cornea than in the midperiphery,5 conjunctival hyperemia, and fine corneal opacities.9 There is often severe blepharospasm and moderate conjunctival inflammation—however, the anterior chambers of the eyes are usually free of inflammation, and intraocular pressure is normal.5 The mechanism of microcyst formation is currently unknown. Corneal epithelial stem cells have a long cycle time and are unlikely to be cytarabine-susceptible; however, they bring about more differentiated transient amplifying cells in the basal layer, which divide more frequently and may therefore be vulnerable to cytarabine toxicity. Common ocular symptoms include blurred vision, severe discomfort or burning pain, photophobia,3,5,7 decreased visual acuity, tearing,3,7 and foreign body sensation.3
Treatment Options
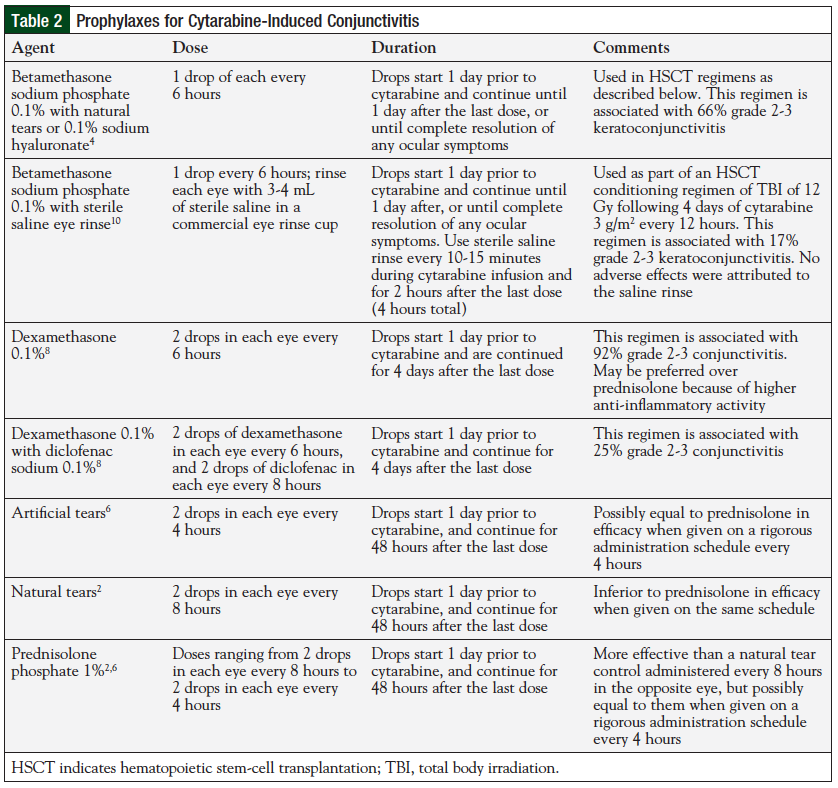
Prophylaxis is generally not recommended at doses <1000 mg/m2.5 Suggested prophylaxis is corticosteroid eye drops5,6,8; however, other agents and combinations have been used successfully.8 These include a variety of preparations, including tear replacement solutions and topical, nonsteroidal anti-inflammatory drops.6,8 Every 4- or 6-hour administration on a strict schedule appears to provide the most benefit, and drops should be continued at least 48 hours after the last cytarabine dose.6 The mechanism of conjunctivitis prevention is unclear, but may rely on a decreased replication rate induced by corticosteroids impacting DNA replication in corneal cells.5 An additional mechanism of action may be a diluting effect on the cytarabine concentration; 1 trial showed benefits achieved from frequent use of artificial tears.6 It is unclear whether components of eye solutions, especially preservatives, can exacerbate the conjunctivitis. Given the limited studies on this toxicity, preservative-free products would be preferred when available.10
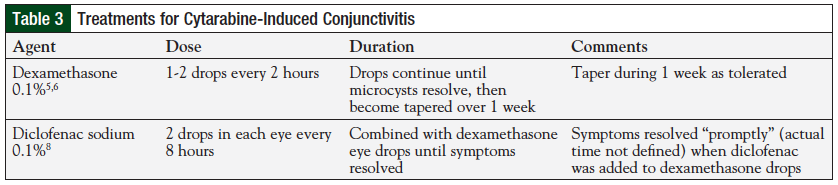
When conjunctivitis occurs there is no standard therapy, and treatment is often left to the local ophthalmologists, who generally apply additional corticosteroid eye drops, with other agents added in as needed.5 See Table 2 for a list of prophylaxes and Table 3 for treatments for cytarabine-induced conjunctivitis. Dexamethasone eye drops are the most common agent used to treat conjunctivitis, and there may be additional benefits derived by adding a topical nonsteroidal anti-inflammatory drug (NSAID).8 Dexamethasone has greater anti-inflammatory activity, and may have better corneal penetration than prednisolone. Pain, irritation, and other symptoms generally respond within days, with visual acuity returning to baseline by 2 weeks, and corneal opacities resolved by 4 weeks.3 Additional symptom benefits may be obtained through the application of cold compresses to the eye, and by keeping lights at a low level.6
Although it has been well-documented for >30 years, cytarabine-induced keratoconjunctivitis continues to be a poorly studied and problematic adverse effect of cytarabine use. Even though evidence has been reported that deoxycytidine, a competitive inhibitor of cytarabine, may be an effective antidote, a commercially available product for patient use is still not available.11 Unless a deoxycytidine product is developed and proven successful, the information currently available would support the addition of an NSAID eye drop to corticosteroids for high-risk or symptomatic patients.8 Additional research is clearly warranted in this area.
References
- Hopen G, Mondino BJ, Johnson BL, et al. Corneal toxicity with systemic cytarabine. Am J Ophthalmol. 1981;91:500-504.
- Lass JH, Lazarus HM, Reed MD, et al. Topical corticosteroid therapy for corneal toxicity from systemically administered cytarabine. Am J Ophthalmol. 1982;94:617-621.
- al-Tweigeri T, Nabholtz JM, Mackey JR. Ocular toxicity and cancer chemotherapy. A review. Cancer. 1996;78:1359-1373.
- Mori T, Watanabe M, Kurotori-Sotome T, et al. Reduced efficacy of topical corticosteroid in preventing cytarabine-induced kerato-conjunctivitis in patients receiving high-dose cytarabine and total body irradiation for allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant. 2008;42:197-199.
- Lochhead J, Salmon JF, Bron AJ. Cytarabine-induced corneal toxicity. Eye (Lond). 2003;17:677-678.
- Higa GM, Gockerman JP, Hunt AL, et al. The use of prophylactic eye drops during high-dose cytosine arabinoside therapy. Cancer. 1991;68:1691-1693.
- Ritch PS, Hansen RM, Heuer DK. Ocular toxicity from high-dose cytosine arabinoside. Cancer. 1983;51:430-432.
- Matteucci P, Carlo-Stella C, Di Nicola M, et al. Topical prophylaxis of conjunctivitis induced by high-dose cytosine arabinoside. Haematologica. 2006;91:255-257.
- Stentoft J. The toxicity of cytarabine. Drug Safety. 1990;5:7-27.
- Mori T, Kato J, Yamane A, et al. Prevention of cytarabine-induced kerato-conjunctivitis by eye rinse in patients receiving high-dose cytarabine and total body irradiation as a conditioning for hematopoietic stem cell transplantation. Int J Hematol. 2011;94:261-265.
- Gococo KO, Lazarus HM, Lass JH. The use of prophylactic eye drops during high dose cytosine arabinoside therapy. Cancer. 1992;69:2866-2867.