Connecting Science to Practice
The core objective of this work was to describe a strategic
approach for devising recommendations that ultimately inform
organizational strategy for improving diversity, equity,
and inclusion (DEI) within the Hematology/Oncology
Pharmacy Association (HOPA). A DEI task force was created
to examine key areas of opportunity and propose recommendations
that aligned with the core pillars of the organization,
and these were prioritized and presented to the
board of directors. The recommendations were aimed at
helping HOPA grow in DEI to better serve its members and
the patients its members serve. The task force evolved into
a committee, and ultimately an advisory group with the goal
of advising the board of directors on priorities and strategies
that ensure integration of DEI across the organization.
In the post-2020 era, individuals, institutions, and organizations have been challenged to confront the long-standing racism and inequity that have systemically plagued our country. Although this challenge is by no means a new one, it has inspired the commitment of time, energy, and resources to address and incorporate diversity, equity, and inclusion (DEI) within institutions and organizations, including healthcare organizations.1 Institutions, organizations, and individuals are responsible and accountable for fostering and maintaining a culture that is diverse, equitable, and inclusive, where their own workforce and membership feel safe and supported in DEI work, as well as in seeking opportunities for engagement and advancement.2 As a healthcare-serving organization seeking to optimize the care of individuals affected by cancer, the Hematology/Oncology Pharmacy Association (HOPA) has a responsibility to its pharmacy members, as well as to the patients that the membership serves.
Diversity in the healthcare workforce, as well as patient-provider racial concordance, optimizes patient outcomes.3 Furthermore, organizational membership and engagement can foster opportunities for career advancement and networking.3 Several factors have been cited for disproportionately low engagement among minoritized groups in organizational opportunities, including lack of mentorship, representation, and sense of inclusion, as well as a potential for implicit preference for White versus Black Americans.4 Despite a recognized need, improvement in diversity among the healthcare workforce has not been realized. Black Americans represent only 3% of oncologists in the oncology workforce, despite representing 13.4% of the American population.5,6 A recent survey in academic emergency medicine over a 6-year span demonstrated that women and racially/ethnically minoritized groups remained less likely to hold leadership positions and are more likely to stay at a lower academic rank than men and well-represented racial/ethnic groups.7 Thus, recognizing the disparities that exist in engagement, leadership roles, and sense of belonging is not enough. Targeted interventions are required to transform organizations that desire equity in membership representation, engagement, and opportunities.
Recognizing this need, we describe herein the steps HOPA has taken to establish a formal strategy to promote DEI within the organization and among the oncology pharmacy community that it represents and serves.
About HOPA
HOPA’s vision is that all individuals with cancer have a hematology oncology pharmacist as an integral member of their care team. To help realize this vision, HOPA’s mission is to support pharmacy practitioners and promote and advance hematology oncology pharmacy to optimize the care of individuals with cancer. HOPA serves more than 3800 members who have expertise in a variety of clinical care settings, representing more than 15 different types of practice sites. Approximately 90% of HOPA members are pharmacists by training. The remaining membership is made up of pharmacy technicians, pharmacy students, and other allied health professionals. HOPA’s core values include leadership, collaboration, integrity, responsiveness, innovation, and caring; these values guide the organization’s work in the 4 key areas of professional development, professional resources and tools, research, and advocacy. We recognize the long-standing systems of racism and inequity that have shaped the experiences of our members and patients, particularly those with diverse backgrounds, beliefs, and lived experiences, and we acknowledge the role that we have in dismantling these systems through action and commitment to the ongoing pursuit of equity and justice.
Call to Action
HOPA’s renewed focus on DEI stemmed from a few notable events, including the 2020 murder of George Floyd, which ignited necessary conversations about systemic racism and inequities that impact marginalized communities; the health disparities observed during the global COVID-19 pandemic that shone an undeniable light on the social determinants of health that, as a result of structural racism, adversely impacted the outcomes of underserved minority communities; the uniting call to pharmacy organizations to pledge support to DEI and condemn discrimination; and, perhaps more important, a clear call from our own membership.
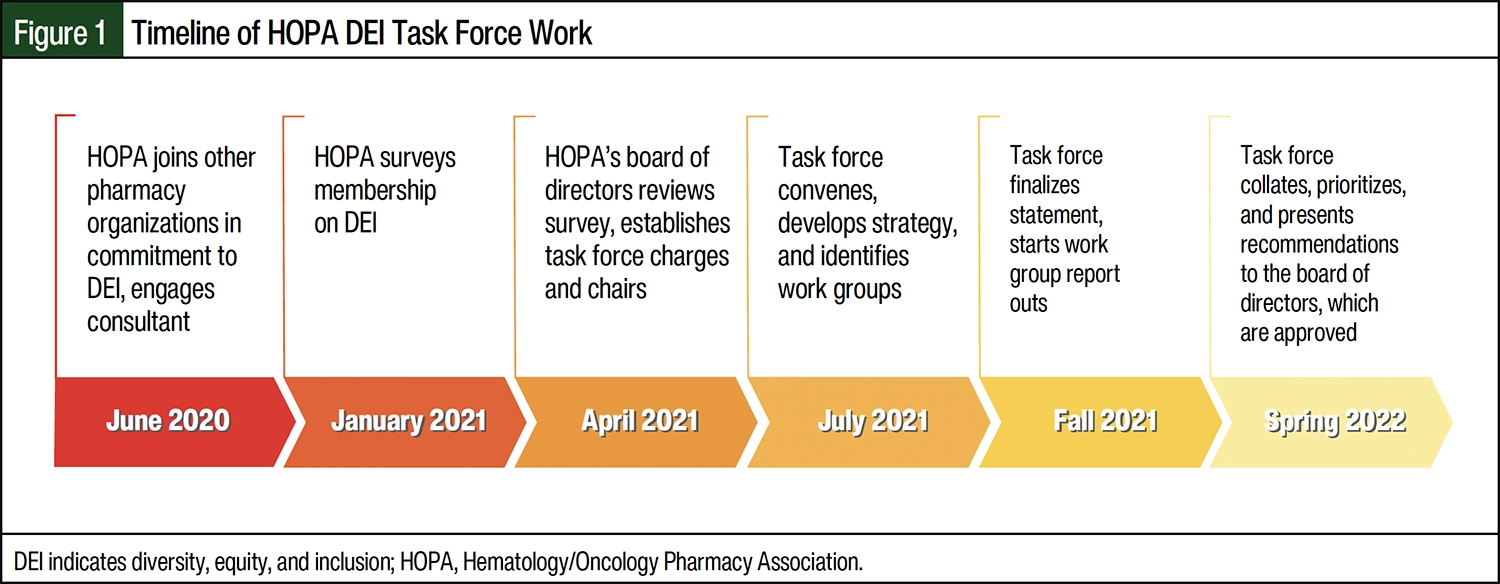
HOPA’s staff and board of directors collaborated with a consulting agency to develop a membership survey centered on DEI. Thereafter, a meeting was convened between the staff and the board of directors to identify concerns and opportunities for improvement. Once member feedback was thematically organized, the board of directors developed a list of charges for what would become the inaugural HOPA DEI Task Force. HOPA aligns each of its task forces and committees to report through 1 of 4 councils. Given the priority that HOPA placed on promoting DEI, this task force was made an executive-level task force, meaning that it reported directly to the board of directors. The president of HOPA committed to serving as the board liaison for the task force, highlighting its organizational priority. A timeline of events for the HOPA DEI Task Force is shown in Figure 1.
Organizing the Approach
To erect the DEI task force, the board of directors identified a chair and vice chair to lead the effort. The DEI task force was listed on the HOPA Volunteer Activity Center website, where members could express interest in serving on the task force. After the annual member update of the volunteer activity center’s preferences, the chair and vice chair were provided with a list of applicants who were interested in serving on the DEI task force. The information included a full curriculum vitae that detailed the applicants’ training, professional experience, clinical practice, research, and teaching experiences. Each applicant also detailed why they were interested in serving on the DEI task force.
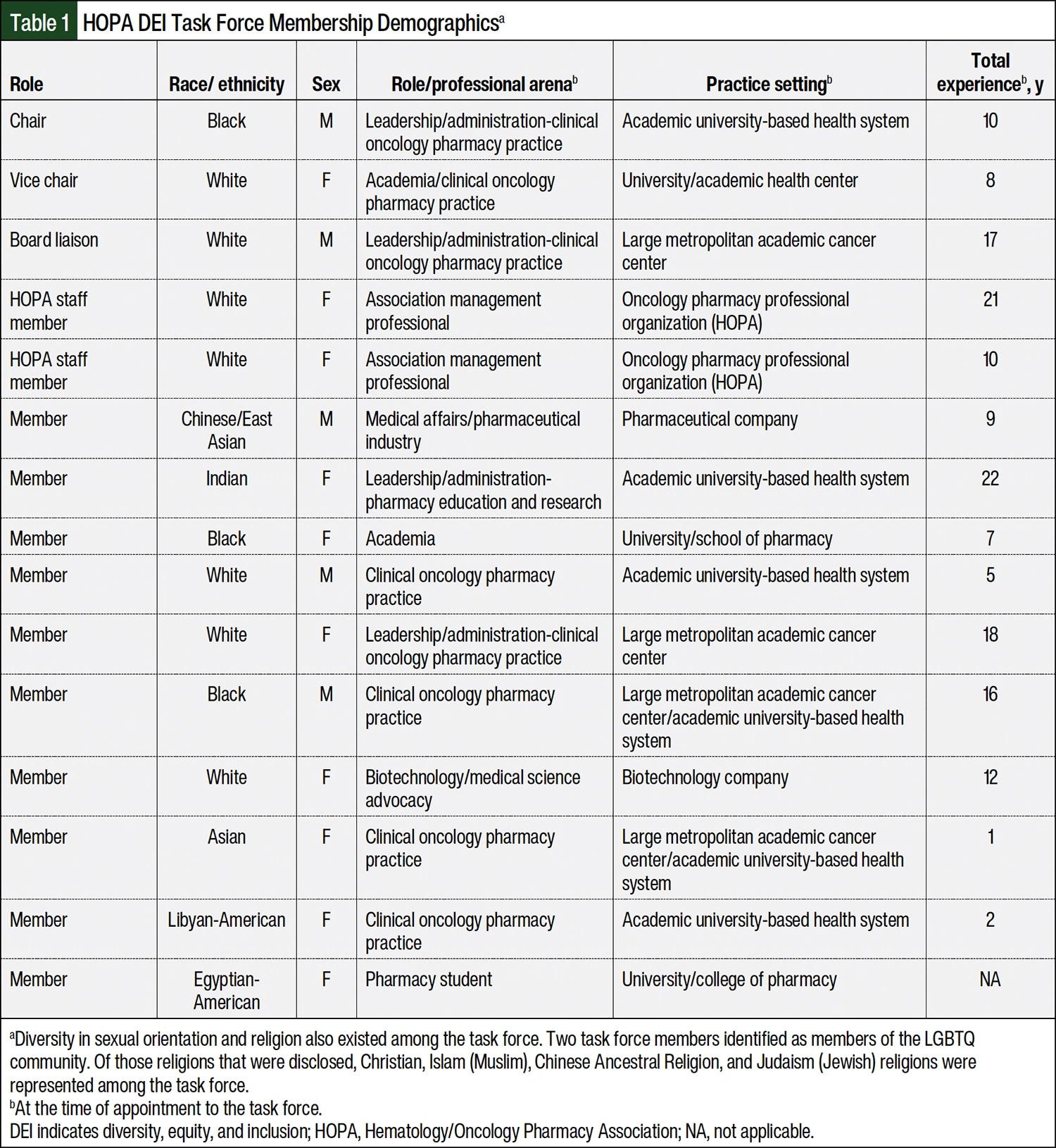
The chair and vice chair were tasked with identifying a total cohort of 10 members. The chair and vice chair felt it critically important that the makeup of the task force reflect the very priorities that it would ultimately be promoting, diversity and inclusion. Thus, they placed particular emphasis on crafting a cohort that had broad representation among the professional pharmacy community, including consideration of race/ethnicity, sex, sexual orientation, clinical practice setting, professional role (eg, academia, clinical practice, pharmaceutical industry, managed care, pharmacy practice leadership), religion (when disclosed), and level of professional experience (Table 1). Considering the valuable perspective of pharmacy trainees, the task force included a pharmacy student and a pharmacy resident member.
All invited members accepted the invitation to participate. On initiation, the chairs, and later the full task force, were given access to the outcome of the membership climate survey, as well as documents and materials that summarized the key findings from the consultant engagement. Those documents, along with the charges issued by the board of directors, served to guide the priorities for the task force. The task force’s primary role was to organize a comprehensive approach to visible, meaningful, and impactful efforts regarding DEI and health equity.
Building a Strategy
Because DEI is a broad and encompassing topic, the task force identified a strategic approach to the association’s goals and initiatives. To begin the strategic planning process, it was imperative to use data from the member survey and the broader cultural climate to ensure that the approach was contemporary and relevant. First, the task force drafted a DEI mission statement, with the goal of intentional inclusion.8 The statement outlined the relevance of DEI to the organization’s work, an acknowledgement of the responsibilities the organization had to address inequities, and a clear commitment to action. Although models exist for crafting such statements, it is important to consider the organization’s infrastructure and membership.9 The DEI mission statement was drafted in alignment with HOPA’s core pillars of professional practice, education, research, and advocacy.8 These pillars represent the 4 overarching councils under which all other HOPA task forces, committees, and working groups fall.8 Alignment with these pillars ensured that all downstream DEI work fit into the core priorities for the organization, and that the work of DEI touched every single working body within the organization. The statement was ultimately reviewed and approved by the board of directors and served as the core anchor for the work that would follow.
To ensure that the task force was aligned on its core priorities, all members reviewed the climate survey results and key findings from the consultant engagement. The group then engaged in a brainstorming session using a virtual collaboration tool, Miro (Miro; Amsterdam, NL), that allowed all members to identify and post what they felt were key priorities and opportunities for HOPA to improve DEI. All ideas were aligned with 1 of the 4 pillars. The task force then divided into 4 smaller workgroups (1 for each core pillar), each of which was tasked with devising recommendations for DEI initiatives that aligned with their respective pillar or council. This work was conducted over the course of several months.
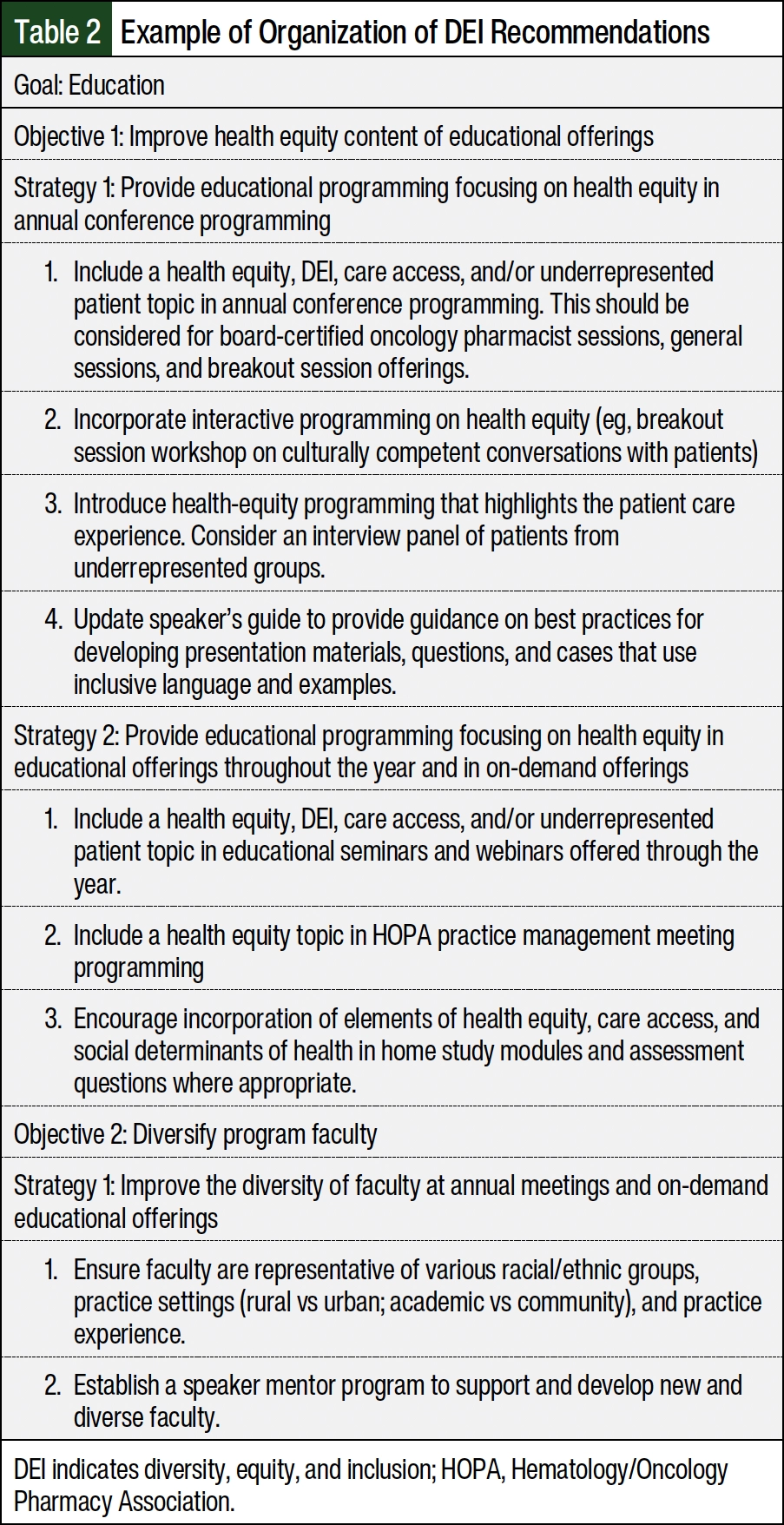
The task force convened for monthly meetings and each smaller working group met in between the monthly task force meetings to work through the recommendations. At each task force meeting, a different working group provided a report of its recommendations, which allowed for the larger task force to engage in discussion and provide feedback on the proposed recommendations. The recommendations were formed to highlight the overarching pillar or council to which they aligned as the goal, followed by an objective and a list of strategies, as outlined in Table 2.
Along the way, the task force chairs presented a midpoint update and the final recommendations to the board of directors. Given the breadth of the final recommendations, the board of directors recommended that the task force prioritize the recommendations. To achieve this, Miro was used to conduct an effort/impact assessment for each recommendation. This tool contained 4 quadrants: low effort/high impact, high effort/high impact, low effort/low impact, and high effort/low impact (Figure 2). Each recommendation, which was coded to reflect the respective goal, objective, and strategy, was placed in the quadrant that the task force felt was most appropriate. Using the tool allowed the task force to visually represent the effort necessary to deliver on each initiative and the associated impact of that initiative.
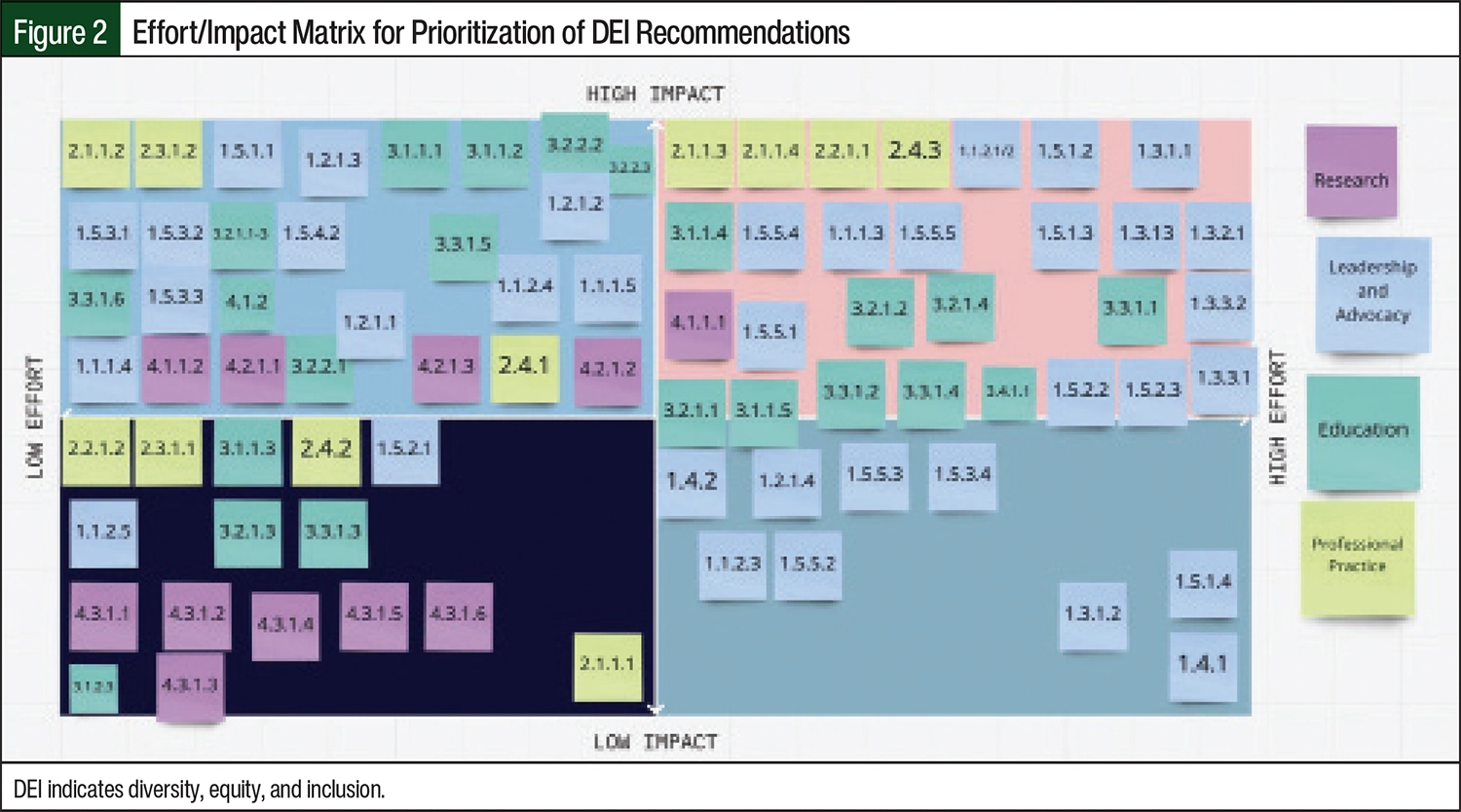
To start, the group tried to focus on a select group of initiatives that were of low-to-moderate effort but moderate-to-high impact. The thought behind this selection was to build necessary, foundational momentum around DEI initiatives that could then translate into larger, higher-effort, higher-impact work over the next 2 to 5 years. Each recommendation was mapped back to the list of recommendations for ease of reference for the incoming DEI committee. Ultimately, the recommendations were finalized and approved by the board of directors.
Discussion
The success of the pivotal and inaugural year of the task force hinged on a number of priorities and commitments from task force members as well as HOPA leadership. First, we composed a task force that was representative of the HOPA organization as a whole. These individuals were representative based on race, sex, religious beliefs, and sexual orientation, and they also represented all aspects of pharmacy practice at varying stages of their careers and practice areas. Each individual brought his or her unique perspective and motives for tackling DEI issues within HOPA and the profession, which contributed to rich, and sometimes raw, discussions. More important, each member of this task force was committed to promoting a safe, judgment-free environment, which allowed the members to be courageous and vulnerable with the mutual understanding that each person’s DEI journey is unique and still in development.
With the composition of the task force set, our main aim for the inaugural year was to build a strong foundation for the future, which began with establishing our DEI statement. HOPA leadership’s commitment to embracing the pain, frustration, and even anger felt within the membership regarding our current DEI efforts and this task force’s courage to challenge the status quo were critical to our success. The commitment and support from HOPA’s board of directors were communicated and displayed in organized action. The task force was established as an executive-level committee that reported directly to the board of directors. In addition, HOPA’s president served as the board liaison, and HOPA’s executive director provided committed support to the task force. This structure reinforced the work of the task force as a key priority.
Improving DEI in any organization requires ongoing commitment. One of the challenges of the task force was ensuring that our proposed recommendations considered a broad set of factors relating to diversity and equity while scoping the recommendations such that feasible and actionable initiatives could be developed for implementation. This generated rich discussion that the task force had to fit into a 1-hour meeting each month. Within HOPA, when a task force is erected, it can either be sunset once it has completed what it was charged to do, or, if a need is identified, it can transition into a full committee that implements the recommendations, initiatives, and strategies proposed by the task force. Considering the breadth and depth of the work needed to improve DEI in a meaningful way, one recommendation of the task force was to transition it into a committee so that the work could continue. HOPA’s board of directors supported the proposal and elected to officially transition the task force into a formal committee. The chair of the task force assumed an immediate past chair role on the committee, and 2 of the task force members were appointed the chair and vice chair of the committee.
Several members of the task force continued their membership on the committee to ensure adequate continuity and background perspective for early initiatives, and a number of new members were appointed to the committee to also ensure that fresh perspectives were incorporated into the ongoing work. Some examples of outputs from the DEI committee include the initiation of demographic data collection of HOPA membership to track representation across membership, committees, and leadership roles to be able to address underrepresentation with targeted efforts; a formal partnership with PharmGradWishList, which involves an annual scholarship to improve racial and ethnic representation of pharmacy trainees at HOPA’s annual conference, as well as the amplification of diverse voices at conferences; the launch of a dedicated landing page on HOPA’s website devoted to DEI resources; updated board member applications to include an assessment of each candidate’s commitment to and experience in promoting DEI; and educational programming dedicated to advancing DEI at annual meetings.
After a year of work as a committee, the organization underwent restructuring aimed at streamlining the committees and working groups to better align work and allow support from the organization management company and board of directors. This effort aligned with a planned refresh of HOPA’s strategic plan, which was amended to include the 2 new core values of inclusion and diversity and a new pillar of organizational excellence. The incorporation of diversity and inclusion as core values allowed for the tenets of DEI to serve as guiding principles for the new strategic plan and will be implemented throughout.
Given that the recommendations coming from the committee could have implications for the work of various other committees and the board of directors, a decision was made to convert the committee into an advisory group, whose purpose is to advise the board of directors on priorities and strategies to charge the work of DEI across the existing structure of committees and initiatives. In doing this, the goal is to embed the work of DEI pursuit within the multifaceted approach to organizational governance rather than as an isolated, stand-alone pursuit of a single committee.
Conclusion
The beginning of 2024 marked 3 years of HOPA’s DEI initiatives. With the changes of the organization and a new strategic plan in place, HOPA re-engaged with its DEI consultant at the end of 2023 to review the accomplishments in DEI and to strategize future DEI efforts. Although much has been accomplished, there is still a lot left to do. HOPA and its members, board, and committees will continue to learn and improve for our pharmacists and our patients.
Dr Alexander is an employee of and owns stock in Merck & Co, and the opinions or perspective expressed herein do not represent the opinions or perspective of his current employer; Dr Buie is an employee of Daiichi Sankyo and has received honoraria for being on an advisory board of Pfizer; Dr Chow is an employee of Orca Bio; Dr Abousaud has received honoraria from PowerPak; Dr Tombleson is an employee of Daiichi Sankyo; Dr Prescott is an employee of Daiichi Sankyo and has received honoraria for being on an advisory board at BeiGene, Janssen, and TerSera Therapeutics; Dr Burton is an employee of and owns stock in AstraZeneca and has received honoraria from the Oncology Nursing Society; Dr Frimpong is an employee of Bayer Pharmaceuticals; Dr Rao, Dr Chen, Dr Autry, Dr Salib, Ms Krolikowski, Ms Stelpflug, and Dr Brown have no conflicts of interest to report.
References
- Stanford FC. The Importance of diversity and inclusion in the healthcare workforce. J Natl Med Assoc. 2020;112:247-249.
- Arya V, Butler L, Leal S, et al. Systemic racism: pharmacists’ role and responsibility. Am J Pharm Educ. 2020;84:8428.
- Allen JM, Abdul-Mutakabbir JC, Campbell HE, Butler LM. Ten recommendations to increase Black representation within pharmacy organization leadership. Am J Health Syst Pharm. 2021;78:896-902.
- Campbell HE, Hagan AM, Gaither CA. Addressing the need for ethnic and racial diversity in the pipeline for pharmacy faculty. Am J Pharm Educ. 2021;85:8586.
- 2021 Snapshot: State of the Oncology Workforce in America. JCO Oncol Pract. 2021;17:249.
- Winkfield KM, Levit LA, Tibbits M, et al. Addressing equity, diversity, and inclusion of Black physicians in the oncology workforce. JCO Oncol Pract. 2021;17:224-226.
- Linden JA, Baird J, Madsen TE, et al. Diversity of leadership in academic emergency medicine: are we making progress? Am J Emerg Med. 2022;57:6-13.
- Hematology/Oncology Pharmacy Association. Diversity, equity and inclusion statement. Accessed March 7, 2025. www.hoparx.org/documents/34/HOPA_DEI_Statement.pdf
- Gentle-Genitty C, Merrit B, Kimble-Hill AC. A model for crafting diversity, inclusion, respect, and equity (DIRE) policy statements toward catalyzing organizational change. ACS Cent Sci. 2021;7:383-391.


