Symptom Overview
The herpes simplex virus (HSV) is in the Herpesviridae family and is primarily associated with blisters or sores in the oral and/or genital mucosa.1 In addition to mucosal damage and pain, HSV reactivation can decrease the patient’s intake of food and fluids and increase the risk for superinfections caused by bacteria or fungi.2 Although mucosal lesions are common in active HSV infection, cutaneous infection may also occur in other areas of skin and, as herpetic whitlow, around the nails and eyes, further increasing morbidity.1
Etiology
Hematopoietic stem-cell transplant (HSCT) recipients are at substantial risk for severe HSV infection or reactivation. Approximately 80% of stem-cell transplant recipients who are seropositive for HSV are at risk for HSV infection and reactivation without proper prophylaxis.3
Allogeneic HSCT recipients have a higher risk for HSV reactivation than recipients of autologous HSCT, because of the necessity for immunosuppressants use in allogeneic HSCT.3 In the first month of receiving HSCT, neutropenia and the breakdown of the mucosal barrier predispose patients to HSV infection and reactivation.3
The risks for HSV infection and reactivation remain during the post–engraftment period, in which cell-mediated immunity may stay underdeveloped, especially with the use of immunosuppressive therapy.3 In general, oral acyclovir or valacyclovir are indicated as prophylactic agents against HSV reactivation in seropositive transplant recipients.4 For patients who cannot take oral medications, intravenous (IV) acyclovir can be administered as prophylaxis.5 Although antiviral prophylaxis can reduce the incidence of reactivation from 80% to 5%, resistance to treatment and poor bioavailability of oral acyclovir can occur.3,6
When patients undergoing HSCT have HSV lesions while receiving HSV prophylaxis, the prophylactic dosing of acyclovir or valacyclovir is typically switched to a treatment dosing. However, resistance can occur in some patients. Acyclovir-resistant HSV infection is an emerging issue in patients who have undergone HSCT. In a prospective observational single-center study of 268 patients who have undergone HSCT, 15% of patients had HSV type-1 isolates identified, and 28% of these patients had acyclovir resistance.7 Acyclovir resistance can be attributed to the deficiency of or alterations in viral thymidine kinase and/or DNA polymerase genes.7
Acyclovir-resistant HSV strains are usually susceptible to alternative agents, such as IV foscarnet and IV cidofovir, because of the different mechanisms of action of these agents.8-10 Foscarnet and cidofovir do not depend on viral thymidine kinase for activation and are inhibitors of viral DNA polymerase; however, these agents are associated with significant adverse effects, such as nephrotoxicity.8-10
Assay sensitivity varies between laboratory tests, and it may be inaccurate to define drug resistance by a single antiviral concentration; however, the breakpoints of half-maximal inhibitory concentration of ≥2 µg/mL for oral and IV acyclovir and of ≥100 µg/mL for IV foscarnet are widely accepted.5,11 If no substantial response to therapy occurs after 7 days of acyclovir treatment, or when new satellite lesions appear 3 to 4 days after starting therapy, acyclovir resistance should be suspected.5 In addition, clinicians should consider adherence to oral antiviral prophylaxis or treatment before determining whether the patient has true resistance to oral or IV acyclovir.5
Treatment Options
When resistance to treatment with oral or IV acyclovir or oral valacyclovir is suspected, phenotypic testing of viral isolates should be conducted and alternative agents should be considered. However, the susceptibility results may take a few weeks, depending on the laboratory that is performing the test.12,13 Therefore, decisions on changing to an alternative agent should be based on the acuity of the infection and the patient’s clinical status.
Despite their improved pharmacokinetic properties compared with acyclovir, valacyclovir and famciclovir are not recommended for the treatment of acyclovir-resistant HSV infection because of their structural and chemical resemblance and their cross-resistance. Like acyclovir, valacyclovir and famciclovir depend on activation by HSV thymidine kinase and may not be effective in the setting of HSV thymidine kinase mutation.5,14
The first-line therapy of HSV infection typically includes a course of IV foscarnet, which is a pyrophosphate analog that acts as a noncompetitive inhibitor of viral RNA and DNA polymerases and does not require activation by viral thymidine kinase.4,5 The typical dose of foscarnet is 40 mg/kg every 8 or 12 hours for 14 to 21 days or until resolution of symptoms.9 The dosing frequency may vary, depending on the severity of the HSV infection and on the patient’s renal function. In patients with renal impairment, the foscarnet dose is adjusted based on creatinine clearance (CrCl) in mL/min/kg of body weight, and its use in patients with CrCl of <0.4 mL/min/kg is not recommended.9
Electrolyte imbalances can occur with foscarnet therapy, which can lead to seizures in rare cases. Therefore, electrolytes should be corrected before initiating treatment with foscarnet. To minimize the risk for nephrotoxicity, IV hydration with 750 to 1000 mL of normal saline or 5% dextrose solution should be given before the first dose and concurrently with each dose of foscarnet.9
Patients who are receiving foscarnet should be monitored closely for any signs or symptoms of nephrotoxicity and electrolyte disturbances, such as hypocalcemia, hypomagnesemia, hypokalemia, hyperphosphatemia, or hypophosphatemia.9 In addition, because of the additional hydration associated with each foscarnet dose, clinicians should monitor patients closely for the signs and symptoms of volume overload, particularly among patients with reduced cardiac function.9
Cidofovir, a deoxycytidine monophosphate analog and a thymidine kinase–independent inhibitor of HSV infection, is an off-label alternative treatment to foscarnet in patients with acyclovir-resistant HSV infections.5,15 Several case reports of immunocompromised patients describe cidofovir’s potential role in acyclovir-resistant HSV infections.16-20 However, the prescribing information of cidofovir has a black box warning about dose-limiting nephrotoxicity and neutropenia.15
Cidofovir is administered intravenously at 5 mg/kg body weight once weekly for 2 weeks, then 5 mg/kg body weight once every 2 weeks for 3 doses, with concurrent hydration and probenecid to prevent nephrotoxicity.15,16
Because of its metabolites’ long half-life, IV cidofovir is dosed less frequently than other systemic therapies, which may be convenient in the outpatient setting. The dosing and duration of therapy of IV cidofovir, which were originally established by LoPresti and colleagues for the treatment of acyclovir- and foscarnet-resistant HSV infection,21 have also demonstrated efficacy in a subsequent case report.16
The use of cidofovir is contraindicated in patients with preexisting renal impairment, such as serum creatinine >1.5 mg/dL, CrCl ≤55 mL/min, or urine protein ≥100 mg/dL (≥2+ proteinuria).15 If serum creatinine increases by 0.3 to 0.4 mg/dL above baseline during therapy, the cidofovir dose should be reduced to 3 mg/kg.15
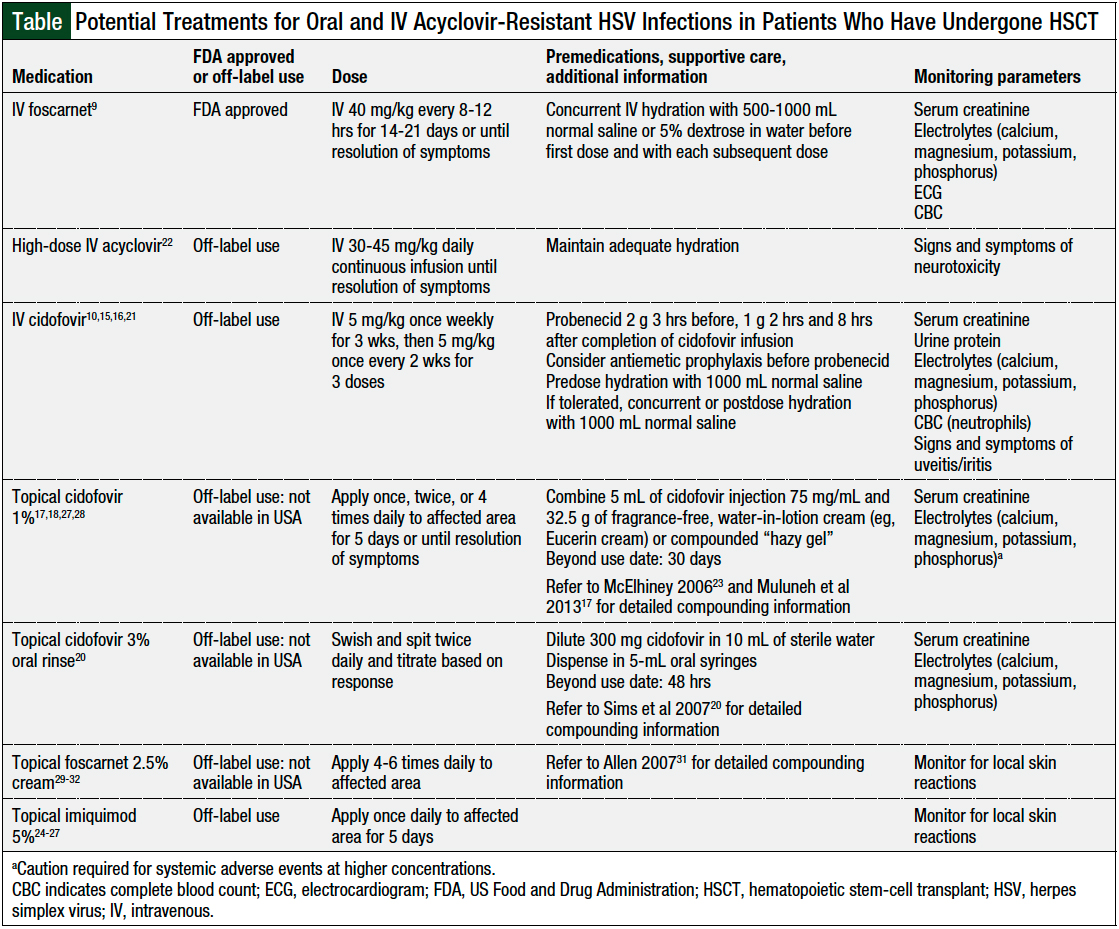
Treatment alternatives to IV foscarnet in patients with acyclovir-resistant HSV infection include IV cidofovir, high-dose IV acyclovir, topical cidofovir, topical imiquimod, and topical foscarnet (Table).9,10,15-18,22-32 However, as noted in the Table, these alternative treatments are used off-label for this indication.9,15,22,24
Although ganciclovir has activities against HSV-1 and HSV-2 similar to acyclovir, it is only FDA approved for the treatment of cytomegalovirus infections.33 In addition, ganciclovir should not be used for acyclovir-resistant HSV infections, because of cross-resistance. Ganciclovir and acyclovir share the same mechanism of resistance, which involves deficiency in intracellular phosphorylation required for drug activation.14 These alternative agents have not been compared in head-to-head studies and should be tailored to the patient’s clinical status and organ functions, particularly renal function.
The use of high-dose IV acyclovir has been reported by Kim and colleagues in a retrospective case series describing 6 patients who had HSCT and received daily acyclovir 30 to 45 mg/kg as continuous IV infusion, with or without concurrent foscarnet, until the resolution of symptoms.22 The researchers aimed to overcome the poor bioavailability of oral acyclovir with the IV route of administration.22 Compared with intermittent dosing, continuous IV acyclovir dosing is preferred in acyclovir-resistant HSV infection, as demonstrated in another case series that showed favorable clinical and virologic responses.34
Kim and colleagues concluded that high-dose IV acyclovir may be a viable alternative for patients with acyclovir-resistant HSV infection who are nonresponsive to or are intolerant of standard treatment dose of oral or IV acyclovir, foscarnet, cidofovir, or ganciclovir.22 Although no significant adverse events were observed with high-dose IV acyclovir, treatment with high-dose IV acyclovir may cause nephrotoxicity and neurotoxicity, such as confusion, lethargy, and hallucinations.22 Clinicians should exercise caution when administering high-dose IV acyclovir to patients with underlying renal impairment.35
Topical therapies may be beneficial in patients who have underlying renal dysfunction or who are at risk for toxicities from the systemic options. The successful (off-label) use of topical cidofovir has been reported in several case reports of patients undergoing HSCT with acyclovir-resistant perianal or orofacial HSV infections.17,18,20,36 These case reports describe various dosing frequencies and durations of cidofovir gel or cidofovir oral rinse.17,18,20,36 A frequently reported concentration for topical cidofovir gel is 1%, and various dosing frequencies have been reported in patients who have undergone HSCT and in patients with AIDS who received topical cidofovir once daily, twice daily, or every 6 hours for 5 days or until resolution of symptoms.17,27,28,36 Higher concentrations (eg, 4%) may cause nephrotoxicity and electrolyte imbalances.17
Topical cidofovir 3% oral rinse formulation has also been used with success.20 In this case report, cidofovir 3% rinse solution was administered as an oral rinse twice daily.20 Although the topical formulations of cidofovir are used off-label and are not commercially available in the United States, they can be compounded from the injectable formulation in accordance with hazardous medication compounding procedures17,20,23 (Table).
Topical imiquimod exerts an indirect antiviral effect via local immune response modification and the induction of host antiviral protein cystatin A.24,37,38 The successful treatment of acyclovir-resistant anogenital HSV infection in immunocompromised patients with topical imiquimod has been reported.25,26,39-41
Although the majority of the data involve patients with HIV infection or patients with cancer who have not undergone HSCT, Martinez and colleagues described the use of imiquimod in a patient with mucocutaneous acyclovir-resistant HSV infection of the mouth, lips, and fingers and a history of mild acute liver graft-versus-host disease (GVHD) who underwent allogeneic HSCT.26 The patient used 5% imiquimod cream 4 times daily in combination with low-dose valacyclovir 500 mg orally daily and reported a complete clearance of lesions within 4 weeks of treatment. Treatment with imiquimod was tapered after 1 month and was discontinued after an additional 3 months.26
The adverse effects of imiquimod treatment can include local skin reactions and the worsening of inflammatory conditions of the skin, including chronic GVHD.24 However, there is a lack of real-world data that demonstrate the impact of imiquimod treatment on patients with GVHD.
Imiquimod formulated in a 5% topical cream is commercially available; however, the dosing for the treatment of acyclovir-resistant HSV infection varies greatly across the literature, ranging from 3 times weekly, every other day, or daily to 4 times daily, partly as a result of the local inflammatory reaction that limits the dosing frequency in some patients.24-27
Topical foscarnet has been predominantly studied in patients with HIV infection, but data are scarce in patients who have undergone HSCT.29,30 One case report describes the use of topical foscarnet in 2 patients with severe acyclovir-resistant HSV infection type-1 stomatitis after allogeneic HSCT.30 The dosing used was foscarnet 2% cream 4 to 6 times daily. The researchers used the formulation that was commercially available in Germany; however, this formulation is used off-label and is currently not commercially available in the United States.30 Compounding instructions are available in the International Journal of Pharmaceutical Compounding for foscarnet 2.5% cream.31 Adverse events associated with foscarnet topical cream, such as skin ulceration, application-site reactions, fever, and headache, have been previously reported in patients with AIDS.32
Discussion
HSV infection poses a major challenge in immunocompromised patients, especially those undergoing allogeneic HSCT.8 With the emergence of acyclovir-resistant HSV infection, new therapeutic approaches are required. Agents that inhibit HSV DNA polymerase, such as foscarnet and cidofovir, may be used in the setting of acyclovir-resistant HSV infection.27 Because of the risk for nephrotoxicity and the dosing requirements, the use of IV foscarnet can be limited in the outpatient setting and may require hospitalization during the initial treatment.
Cidofovir’s long half-life allows for longer dosing intervals, making it a suitable alternative for the outpatient treatment of acyclovir-resistant HSV. However, the therapeutic use of IV cidofovir is limited by neutropenia and dose-limiting nephrotoxicity, which may result in damage to the proximal tubular cells and acute renal failure.15
High-dose IV acyclovir, topical cidofovir, topical imiquimod, and topical foscarnet are alternative or adjunctive therapeutic options for oral or IV standard treatment dose in acyclovir-resistant HSV infections. The available literature in support of these agents is limited to retrospective studies and case reports. The use of high-dose IV acyclovir, topical cidofovir, topical imiquimod, or topical foscarnet is not generally recommended as first-line therapy for acyclovir-resistant HSV infection in patients who have undergone HSCT. However, high-dose IV acyclovir may be considered in patients who do not tolerate other systemic therapy options, such as IV foscarnet or IV cidofovir.
Topical agents should be considered in patients with persistent lesions despite receiving systemic treatment for acyclovir-resistant HSV or in patients who are at risk for significant adverse events from systemic agents. In addition, pharmacists should keep in mind that topical cidofovir and topical foscarnet formulations are not commercially available in the United States and should be compounded extemporaneously (Table).
It is currently unclear why certain patients have acyclovir resistance, although some data suggest that long-term prophylaxis may increase the risk for resistance.42
Conclusion
Although therapeutic options are available for acyclovir-resistant HSV infections, systemic treatments are limited by their clinical and safety profiles. The treatment of acyclovir-resistant HSV infection is an ongoing dilemma in the clinical setting and continues to be a major concern in patients who have undergone HSCT.
In addition to future research on the optimal management of acyclovir-resistant HSV infections, more studies are needed to optimize HSV infection prophylaxis in patients undergoing HSCT.
Author Disclosure Statement
Dr Park, Dr Huang, and Dr Ciccosanti have no conflicts of interest to report.
References
- Grinde B. Herpesviruses: latency and reactivation–viral strategies and host response. J Oral Microbiol. 2013;5:22766.
- Zecha JAEM, Raber-Durlacher JE, Laheij AMGA, et al. The impact of the oral cavity in febrile neutropenia and infectious complications in patients treated with myelosuppressive chemotherapy. Support Care Cancer. 2019;27:3667-3679.
- Young JAH, Weisdorf DJ. Infections in recipients of hematopoietic stem cell transplants. In: Bennett JE, Dolin R, Blaser MJ, eds. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 8th ed. Vol 2. Philadelphia, PA: Saunders; 2015:3425-3439.e5.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Prevention and Treatment of Cancer-Related Infections. Version 2.2020. June 5, 2020. www.nccn.org/professionals/physician_gls/pdf/infections.pdf. Accessed May 9, 2021.
- Bacon TH, Levin MJ, Leary JJ, et al. Herpes simplex virus resistance to acyclovir and penciclovir after two decades of antiviral therapy. Clin Microbiol Rev. 2003;16:114-128.
- Poole CL, James SH. Antiviral therapies for herpesviruses: current agents and new directions. Clin Ther. 2018;40:1282-1298.
- Kakiuchi S, Tsuji M, Nishimura H, et al. Association of the emergence of acyclovir-resistant herpes simplex virus type 1 with prognosis in hematopoietic stem cell transplantation patients. J Infect Dis. 2017;215:865-873.
- Chakrabarti S, Pillay D, Ratcliffe D, et al. Resistance to antiviral drugs in herpes simplex virus infections among allogeneic stem cell transplant recipients: risk factors and prognostic significance. J Infect Dis. 2000;181:2055-2058.
- Foscavir (foscarnet sodium) injection [prescribing information]. Hospira; October 2020.
- Chen Y, Scieux C, Garrait V, et al. Resistant herpes simplex virus type 1 infection: an emerging concern after allogeneic stem cell transplantation. Clin Infect Dis. 2000;31:927-935.
- Piret J, Boivin G. Resistance of herpes simplex viruses to nucleoside analogues: mechanisms, prevalence, and management. Antimicrob Agents Chemother. 2011;55:459-472.
- Afshar B, Bibby DF, Piorkowska R, et al. A European multi-centre external quality assessment (EQA) study on phenotypic and genotypic methods used for herpes simplex virus (HSV) drug resistance testing. J Clin Virol. 2017;96:89-93.
- Labcorp. Herpes simplex virus (HSV) types 1/2 phenotyping for acyclovir drug resistance. www.labcorp.com/tests/138370/herpes-simplex-virus-hsv-types-1-2-phenotyping-for-acyclovir-drug-resistance. Accessed May 6, 2021.
- Reusser P. Herpesvirus resistance to antiviral drugs: a review of the mechanisms, clinical importance and therapeutic options. J Hosp Infect. 1996;33:235-248.
- Vistide (cidofovir injection) [prescribing information]. Gilead Sciences; September 2010.
- Andrei G, Fiten P, Goubau P, et al. Dual infection with polyomavirus BK and acyclovir-resistant herpes simplex virus successfully treated with cidofovir in a bone marrow transplant recipient. Transpl Infect Dis. 2007;9:126-131.
- Muluneh B, Dean A, Armistead P, Khan T. Successful clearance of cutaneous acyclovir-resistant, foscarnet-refractory herpes virus lesions with topical cidofovir in an allogeneic hematopoietic stem cell transplant patient. J Oncol Pharm Pract. 2013;19:181-185.
- Evans KG, Morrissey KA, Goldstein SC, et al. Chronic acyclovir-resistant HSV-2 ulcer in an immunosuppressed patient treated with topical cidofovir. Arch Dermatol. 2011;147:1462-1463.
- Saunders IM, Lahoti A, Chemaly RF, et al. Topical cidofovir-induced acute kidney injury in two severely immunocompromised patients with refractory multidrug-resistant herpes simplex virus infections. J Oncol Pharm Pract. 2016;22:325-331.
- Sims CR, Thompson K, Chemaly RF, et al. Oral topical cidofovir: novel route of drug delivery in a severely immunosuppressed patient with refractory multidrug-resistant herpes simplex virus infection. Transpl Infect Dis. 2007;9:256-259.
- LoPresti AE, Levine JF, Munk GB, et al. Successful treatment of an acyclovir- and foscarnet-resistant herpes simplex virus type 1 lesion with intravenous cidofovir. Clin Infect Dis. 1998;26:512-513.
- Kim JH, Schaenman JM, Ho DY, Brown JMY. Treatment of acyclovir-resistant herpes simplex virus with continuous infusion of high-dose acyclovir in hematopoietic cell transplant patients. Biol Blood Marrow Transplant. 2011;17:259-264.
- McElhiney LF. Topical cidofovir for treatment of resistant viral infections. Int J Pharm Compd. 2006;10:324-328.
- Imiquimod cream USP, 5%, for topical use [prescribing information]. Taro Pharmaceuticals; 2016.
- Perkins N, Nisbet M, Thomas M. Topical imiquimod treatment of aciclovir-resistant herpes simplex disease: case series and literature review. Sex Transm Infect. 2011;87:292-295.
- Martinez V, Molina JM, Scieux C, et al. Topical imiquimod for recurrent acyclovir-resistant HSV infection. Am J Med. 2006;119:e9-e11.
- Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64:1-137. Erratum in: MMWR Recomm Rep. 2015;64:924.
- Lalezari J, Schacker T, Feinberg J, et al. A randomized, double-blind, placebo-controlled trial of cidofovir gel for the treatment of acyclovir-unresponsive mucocutaneous herpes simplex virus infection in patients with AIDS. J Infect Dis. 1997;176:892-898.
- Pechère M, Wunderli W, Trellu-Toutous L, et al. Treatment of acyclovir-resistant herpetic ulceration with topical foscarnet and antiviral sensitivity analysis. Dermatology. 1998;197:278-280.
- Heidenreich D, Kreil S, Mueller N, et al. Topical treatment of acyclovir-resistant herpes simplex virus stomatitis after allogeneic hematopoietic cell transplantation. Oncol Res Treat. 2020;43:672-677.
- Allen LV Jr. Foscarnet 2.5% topical cream. Int J Pharm Compd. 2007;11:509.
- Javaly K, Wohlfeiler M, Kalayjian R, et al. Treatment of mucocutaneous herpes simplex virus infections unresponsive to acyclovir with topical foscarnet cream in AIDS patients: a phase I/II study. J Acquir Immune Defic Syndr. 1999;21:301-306.
- Kimberlin DW, Whitley RJ. Antiviral therapy of HSV-1 and -2. In: Arvin A, Campadelli-Fiume G, Mocarski E, et al, eds. Human Herpesviruses: Biology, Therapy, and Immunoprophylaxis. Cambridge: Cambridge University Press; 2007:chap 64.
- Fletcher CV, Englund JA, Bean B, et al. Continuous infusion of high-dose acyclovir for serious herpesvirus infections. Antimicrob Agents Chemother. 1989;33:1375-1378.
- Zovirax (acyclovir) capsules, tablets, and suspension [prescribing information]. GlaxoSmithKline; June 2005.
- Epstein JB, Gharapetian S, Rejali AR, et al. Complex management of resistant oral herpes simplex virus infection following hematopoietic stem cell transplantation: potential role of topical cidofovir. Support Care Cancer. 2016;24:3603-3606. Erratum in: Support Care Cancer. 2016;24:3607.
- Buck HW. Imiquimod (Aldara cream). Infect Dis Obstet Gynecol. 1998;6:49-51.
- Kan Y, Okabayashi T, Yokota SI, et al. Imiquimod suppresses propagation of herpes simplex virus 1 by upregulation of cystatin A via the adenosine receptor A1 pathway. J Virol. 2012;86:10338-10346.
- Gilbert J, Drehs MM, Weinberg JM. Topical imiquimod for acyclovir-unresponsive herpes simplex virus 2 infection. Arch Dermatol. 2001;137:1015-1017.
- Hirokawa D, Woldow A, Lee SN, Samie F. Treatment of recalcitrant herpes simplex virus with topical imiquimod. Cutis. 2011;88:276-277.
- Lascaux AS, Caumes E, Deback C, et al. Successful treatment of aciclovir and foscarnet resistant herpes simplex virus lesions with topical imiquimod in patients infected with human immunodeficiency virus type 1. J Med Virol. 2012;84:194-197.
- Jiang YC, Feng H, Lin YC, Guo XR. New strategies against drug resistance to herpes simplex virus. Int J Oral Sci. 2016;8:1-6.