Connecting Science to Practice
This study highlights the role of pediatric pharmacists in
establishing clinical practice guideline–consistent antiemetic
therapy in children who have undergone hematopoietic
stem cell transplantation and can be helpful for
other institutions that are interested in adopting a similar
approach. By integrating evidence-based clinical guidelines
from organizations, healthcare teams, including pharmacists,
have optimized antiemetic protocols. A pharmacist-
guided implementation of these protocols demonstrated
significant improvements in emesis control, reduced
reliance on intravenous antiemetics, and aligned practices
with institutional infection prevention goals. This multidisciplinary
approach exemplifies the critical role of translating
scientific research into personalized, patient-centered
care for improved clinical outcomes.
Chemotherapy-induced nausea and vomiting (CINV) is one of the most immediately disruptive adverse events (AEs) associated with hematopoietic stem cell transplantation (HSCT). The high-dose, multiday, multidrug, alkylating agent–heavy composition of the conditioning regimens, often incorporating total body irradiation (TBI), contribute to substantial nausea and vomiting morbidity in the acute and delayed phases of treatment.1,2 Despite receiving prophylaxis with a 5-hydroxy-tryptamine 3 (5-HT3) antagonist with or without dexamethasone, complete control of nausea and vomiting in children undergoing HSCT remained low at 5% and 12% in the acute and delayed phase, respectively.1 In addition to a diminished quality of life (QOL), nausea and vomiting may negatively impact patients’ transplant trajectories because of a longer duration of initial hospital stays, readmission for symptom management, increased utilization of intravenous (IV) therapies, and a higher reliance on parenteral nutrition (PN).3-5 Nausea and vomiting may also lead to poor oral nutrition, which has been correlated with increased rates of severe graft-versus-host disease (GVHD).6
Advancements in our understanding of the underlying mechanisms of CINV have facilitated significant progress in its treatment and yielded new therapeutics. Established clinical practice guidelines (CPGs) from ASCO and the Pediatric Oncology Group of Ontario (POGO) recommend a 3-drug combination of a 5-HT3 receptor antagonist, a neurokinin-1 receptor antagonist, and dexamethasone for CINV prophylaxis in children receiving highly emetogenic chemotherapy.7,8 Drug-drug and drug-disease interactions preclude safe administration of the 3-drug combination in subsets of patients undergoing a transplant.9-11 The incorporation of novel agents, such as olanzapine, in the treatment of pediatric CINV has provided regimen flexibility while maintaining safety and efficacy.12 However, the reported use of olanzapine for CINV has been limited to children aged ≥3 years.13 Because these new modalities to optimize CINV have concomitant limitations and drawbacks, a holistic approach to critically evaluate and optimize antiemetic therapy that accounts for drug interactions, disease-based contraindications, and the patient’s past experience is needed.
This study described the implementation of a pharmacist-guided, CPG-consistent protocol for nausea and vomiting control in children receiving chemotherapy with or without TBI conditioning before HSCT. To measure the impact of this protocol implementation, we compared emesis control, the use of IV antiemetics, and PN before (prephase) and after (postphase) the implementation of the protocol.
Methods
The Pediatric Blood and Marrow Transplant Program at Seattle Children’s Hospital is a consortium between the hospital and Fred Hutchinson Cancer Center (FHCC). The conjoined program performs an average of 70 blood and marrow transplants annually. Outpatient and inpatient transplant teams consist of attending physicians, advanced practice providers, nurses, pharmacists, and nutritionists. We have 2 dedicated clinical pharmacists in each outpatient and inpatient setting with comprehensive knowledge regarding the special pharmacotherapeutic needs of pediatric transplant patients. They work side-by-side with the multidisciplinary medical team, fulfilling various roles and responsibilities as described in 2018 by the American Society for Blood and Marrow Transplantation (now American Society for Transplantation and Cellular Therapy) Pharmacy Special Interest Group.14 Because of the extreme complexity of care in this population, pharmacists provide thorough medication education to each patient and/or their family before admission for transplant and again on discharge. Each patient and/or their family is counseled on chemotherapy, immunosuppressants, anti-infective drugs, antiemetic drugs, and any other medications prescribed throughout their transplant course to ensure understanding and compliance with an exceptionally substantial number of medications.
Before August 2019, antiemetic prophylaxis for post-HSCT chemotherapy with or without TBI was exclusively scheduled as IV ondansetron. Breakthrough nausea and vomiting was managed by increasing the frequency of ondansetron administration, and/or by adding combinations of other antiemetics, including diphenhydramine, metoclopramide, or lorazepam. Most of these medications were administered intravenously. Despite the often-around-the-clock antiemetic therapy, emesis control was suboptimal in most patients and frequent access of the central line was misaligned with our institution’s effort to decrease central line–associated bloodstream infections.
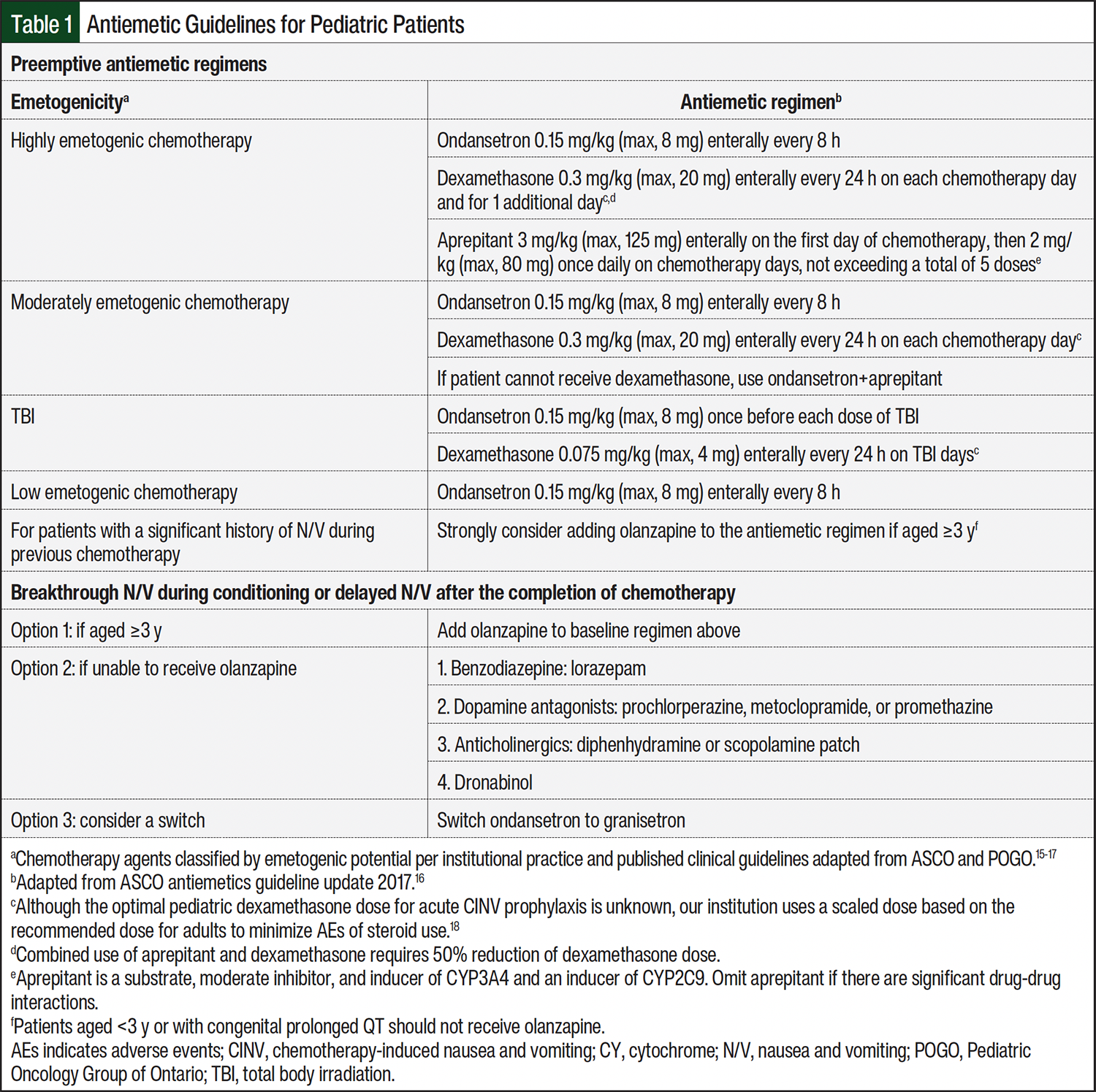
In 2018, a team of HSCT attending physicians and pharmacists discussed the best approach to apply the ASCO and POGO antiemetic guidelines15,16 to pediatric patients undergoing HSCT at our institution. We revised our antiemetic protocol to be consistent with these guidelines and agreed on a backbone for all conditioning regimens with enteral-administered ondansetron, adding prophylactic dexamethasone and/or aprepitant based on the emetogenic potential of each chemotherapy with or without TBI on every day of the conditioning regimen (Table 1).15-18 We identified several circumstances where dexamethasone would be omitted or replaced with aprepitant if not already prescribed, such as when a patient is receiving a T-cell–depleted HSCT regimen where infection risk is already high and dexamethasone may further increase the risk9; when patients are receiving a regimen with posttransplant cyclophosphamide to target GVHD where the immunosuppressive property of dexamethasone may interfere with proliferation of allo-reactive T cells and compromise the efficacy of posttransplant cyclophosphamide10; or when a patient is already receiving steroids. Our infectious disease service also documented the recommendation to omit dexamethasone as an antiemetic if the patient had a recent invasive fungal disease or other serious infection in the pretransplant consult.
Aprepitant is a substrate, a moderate inhibitor, and an inducer of cytochrome (CY)P3A4. Aprepitant is also an inducer of CYP2C9, and therefore is associated with a significant number of drug interactions.11 Aprepitant was allowed in patients aged ≥6 months if they were not receiving concomitant contraindicated medications or if the effect of any drug-drug interactions could be clinically managed by close monitoring or dose adjustment according to the prescribing information or drug review publications.11,19,20 In regards to chemotherapy specifically used in conditioning regimens, aprepitant could be coadministered with busulfan only if there was therapeutic drug monitoring.21 However, concomitant use of aprepitant with thiotepa was avoided because of concern for reduced exposure of tepa, an active thiotepa metabolite.22
The revised institutional protocol was evaluated and approved by the FHCC Standard Practice committee. All frontline staff, including attending physicians, advanced practice providers, nurses, and pharmacists, received discipline-specific education via in-person or virtual group teaching sessions. The appropriate antiemetic therapy based on the emetogenicity of each day’s chemotherapy TBI was integrated into each conditioning regimen order set in the electronic health record (EHR) system. To further ensure adherence to this newly established protocol, the pharmacist interviewed patients and/or their families regarding the efficacy and intolerance of previous antiemetic use in their pretransplant appointments. The pharmacist then assessed any drug-drug or drug-disease interactions and documented a patient-specific antiemetic plan in the EHR explaining any omissions or substitutions according to Table 1. The pharmacist’s documentation also included first- and second-line agents for the treatment of breakthrough nausea and vomiting. As part of the chemotherapy ordering workflow, providers referred to the pharmacist’s recommendation and ensured that the antiemetic therapy was ordered as recommended. All patients received enteral antiemetics at admission, and IV antiemetic formulations were allowed if they were intolerant to enteral antiemetic drugs. The protocol was implemented in August 2019.
We included all consecutive patients who underwent autologous or allogeneic transplantations with conditioning regimens containing chemotherapeutic agents with or without TBI at our institution from May 2018 to January 2021. Patients in the prephase group received scheduled IV ondansetron at the beginning of conditioning, whereas patients in the postphase group followed an enteral antiemetic regimen, as outlined in Table 1. Patients who received posttransplant treatment with cyclophosphamide were excluded from both groups because of the possible overlap of emesis resulting from pretransplant conditioning versus posttransplant cyclophosphamide.
This study was approved by the Seattle Children’s Hospital Institutional Review Board (IRB). Ethical approval and consent to participate was waived by the IRB because this study was conducted retrospectively from data obtained for clinical purposes.
For the analysis of emesis control and IV antiemetic use, the data were collected from the beginning of conditioning (initiation of chemotherapy or TBI) until 5 days after the end of conditioning. The period for emesis control was divided into 2 phases: acute, which was defined as the period from the start of conditioning until 24 hours after the last chemotherapy or TBI, and delayed, which was defined as the period from the end of the acute phase until 5 days after the last chemotherapy or TBI. PN use was captured after admission and throughout the entire hospitalization period for HSCT. The number of days to PN was determined from the first day of conditioning to the day of PN initiation.
As a measure of emesis control, an emesis-free day was defined as the absence of any charted emesis in the EHR over a 24-hour period. Complete emesis control was defined as the absence of any charted emesis in the EHR over the study period. The charted administration of scheduled and as-needed IV antiemetics was collected. These medications included 5-HT3 antagonists (ie, ondansetron, granisetron), dexamethasone, lorazepam, dopamine antagonists (ie, prochlorperazine, metoclopramide), and diphenhydramine.
Statistical Analysis
The summary statistics are presented as medians and interquartile ranges (IQRs) or numbers and percentages. The differences between the percentages were tested using a 2-sample test for the equality of proportions with continuity correction. The differences between the medians were tested using 5000 bootstrap replications of the difference. Kaplan-Meier survival curves were used to characterize the time-to-event results, such as the days to PN use or the days to emesis. Cox regression was used to compare the days to emesis between the pre- and postphase groups and were adjusted for patient age, which is a known confounder.23 All analyses were conducted using R version 4.3.
Results
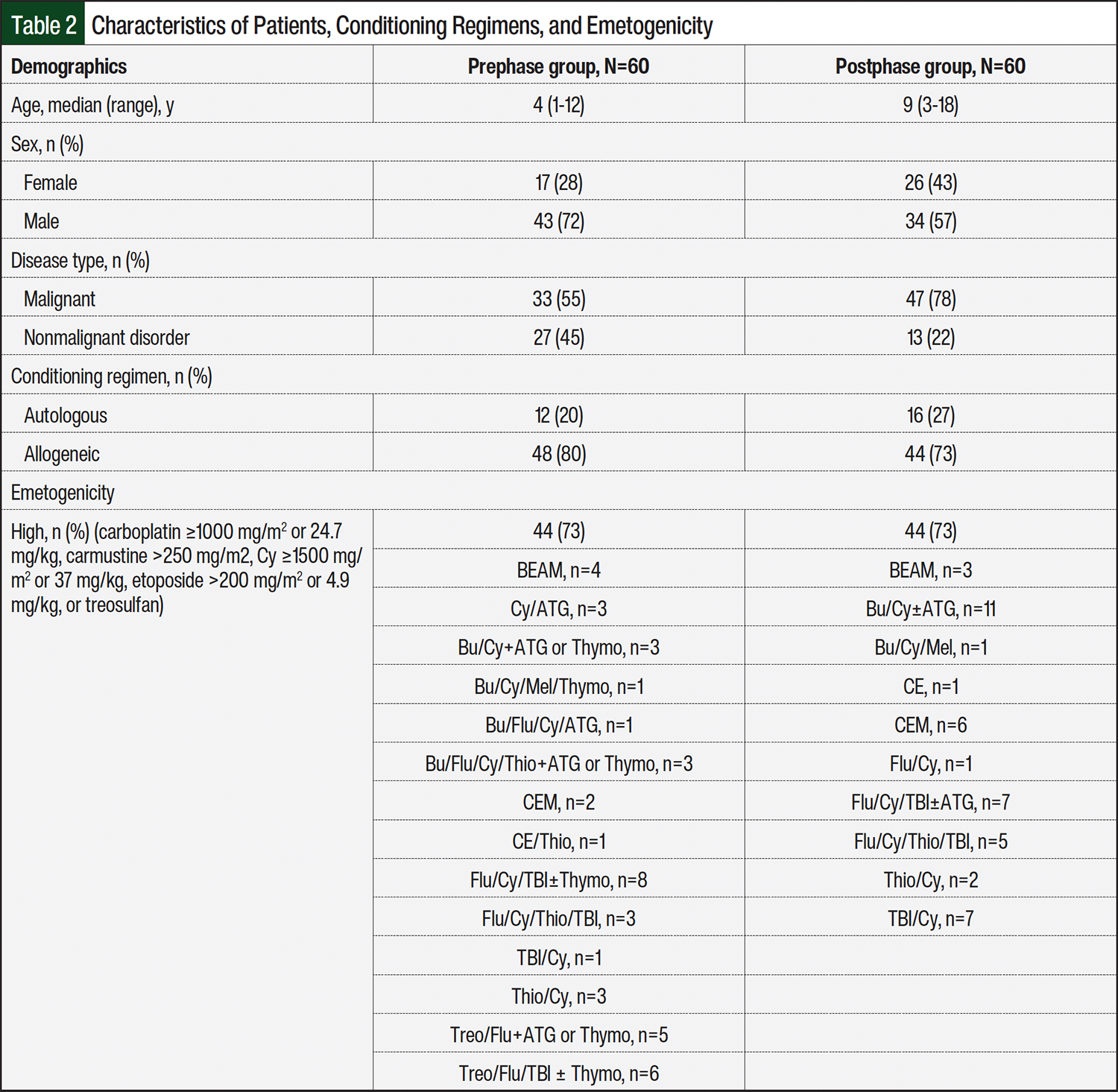
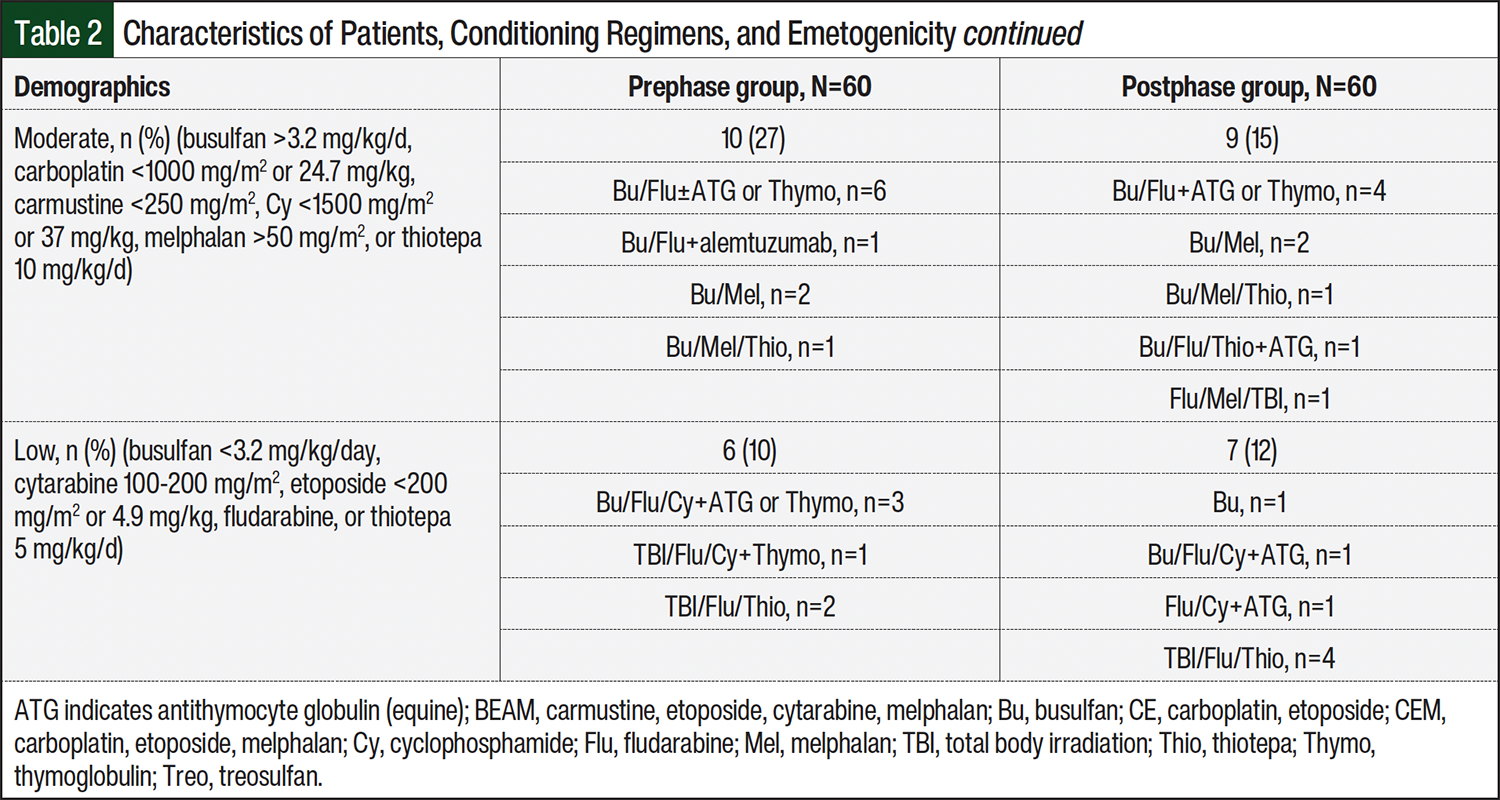
From the time the protocol was implemented in August 2019, 60 consecutive patients who underwent HSCT before guideline implementation were included in the prephase group (May 2018-July 2019). Another 60 consecutive patients who underwent HSCT after guideline implementation were included in the postphase group (August 2019-January 2021). The patients’ characteristics, conditioning regimens, and emetogenicity are summarized in Table 2.
Of the 60 patients in the prephase group, 3 (5%) had complete emesis control compared with 16 (27%) of the 60 patients in the postphase group (P=.002). The median difference in the percentage of emesis-free days between the 2 groups was 13% (95% confidence interval [CI], 0-24). When categorized into acute phase and delayed phase, the differences in the percentage of emesis-free days between the pre- and postphase groups were 14% (95% CI, 4-29) and 25% (95% CI, 0-50), respectively.
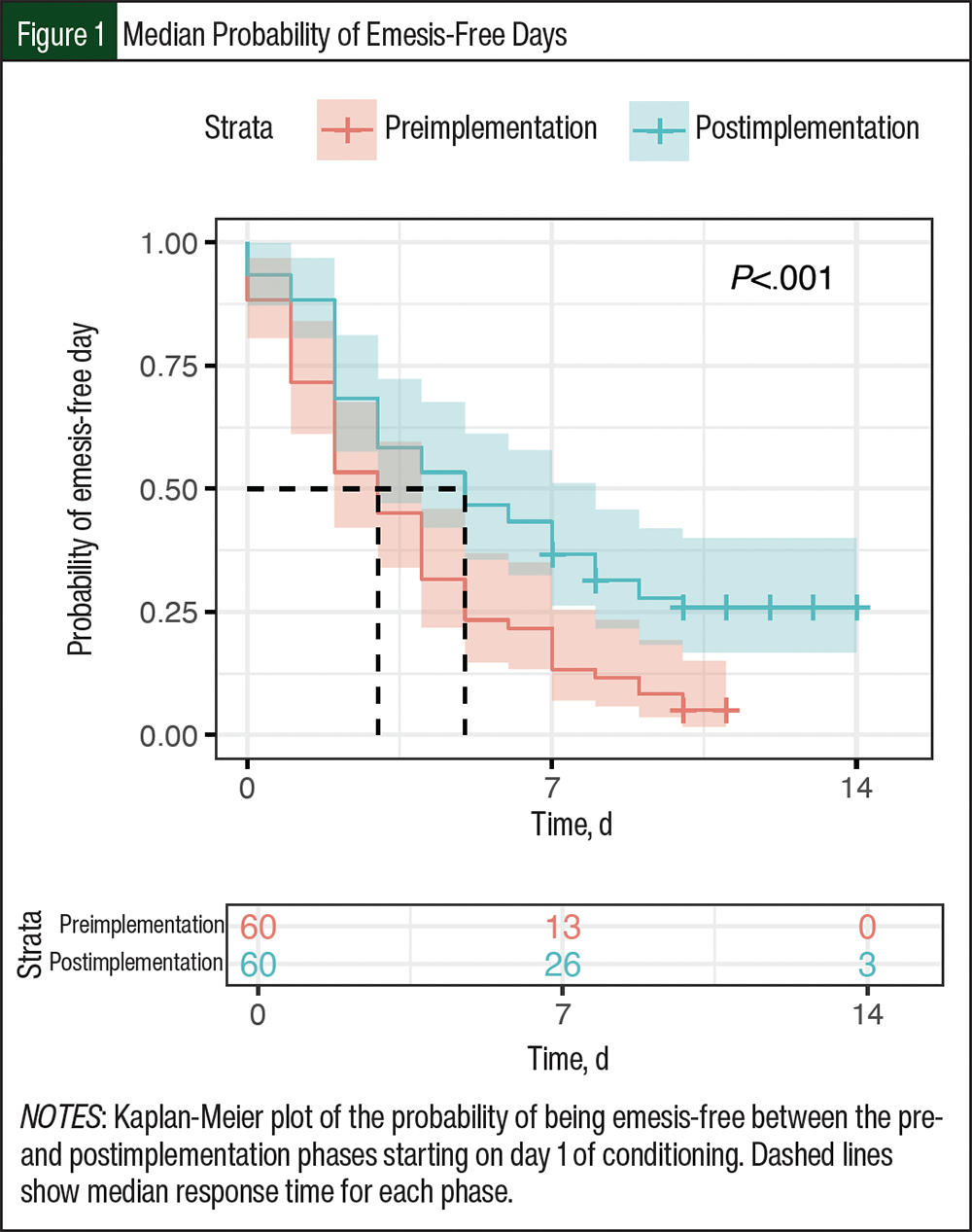
A Kaplan-Meier plot showed that the difference between the 2 groups in median days until emesis was 2 days, with the median of day 3 for the prephase group and day 5 for the postphase group (Figure 1). Although the CIs overlapped somewhat between the 2 groups, the overall difference was significant (P<.001). This pattern was also seen with Cox regression; adjusted by patient age, the hazard ratio for the postphase group compared with the prephase group was 0.47 (95% CI, 0.27-0.84; P=.01).
All 60 patients in the prephase group received ≥1 doses of IV antiemetics, with a median daily dose count of 5.5 (IQR, 4-7.9). Of the 60 patients in the postphase group, 13 (22%) tolerated enteral antiemetics exclusively and 47 (78%) received some form of IV antiemetics, with a median daily dose count of 1.3 (IQR, 0.1-3.4). Overall, the patients in the postphase group who needed any IV antiemetics received a median of 4.1 (95% CI, 3.0-5.3) fewer daily IV doses than the prephase group.
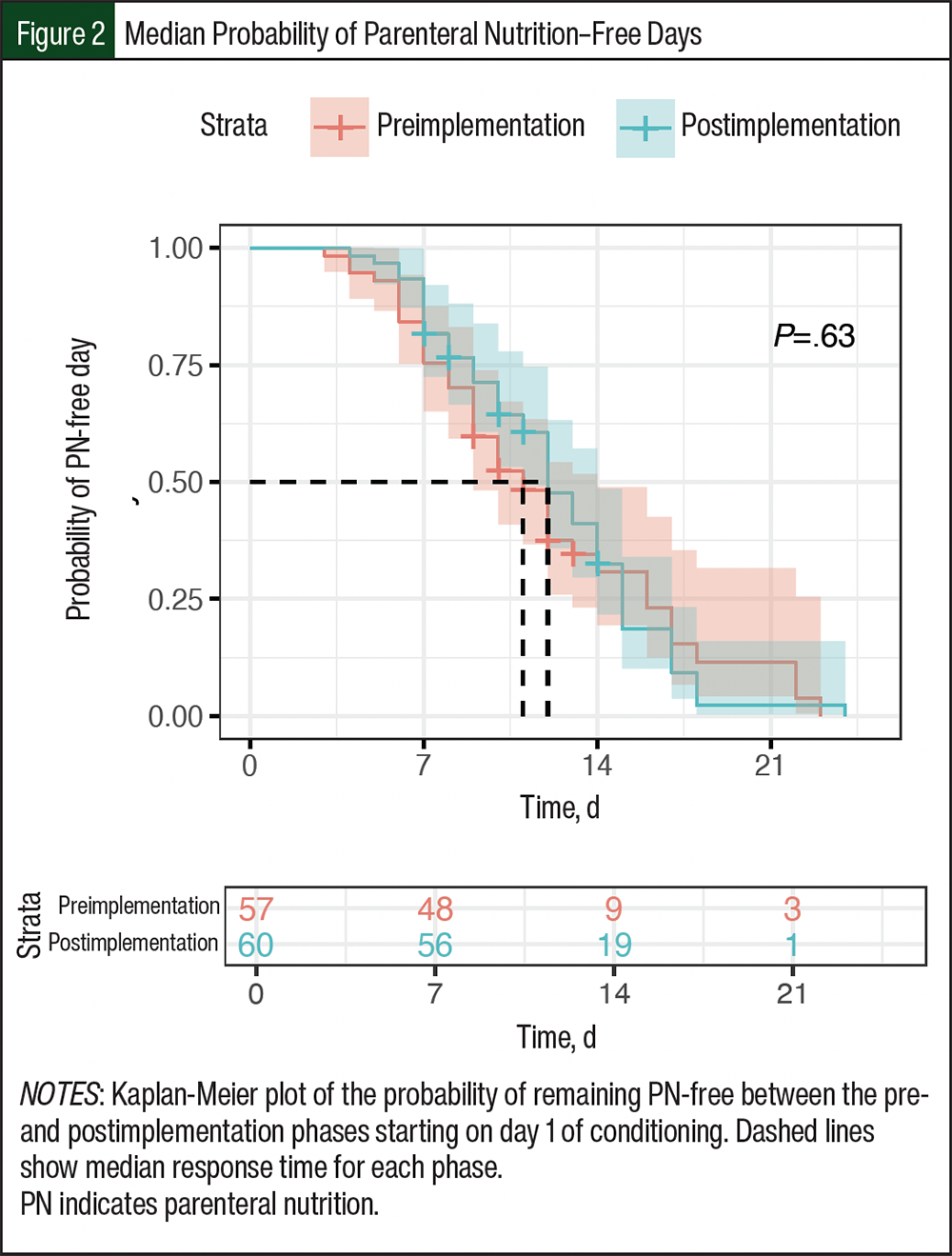
Of the 60 patients in each of the pre- and postphase groups, 46 (77%) and 50 (83%), respectively, received PN, and the difference was not significant (P=.49). The median difference in days to PN between the 2 groups was 3 days (95% CI, 0-4.5). However, a Kaplan-Meier plot showed a median of 1 day later to PN initiation in the postphase group, which was not significantly different from the prephase group (Figure 2; P=.63).
Discussion
Our work highlights the result of implementing CPG-consistent antiemetic therapy in children who receive HSCT, a critical but underreported patient population. All patients in the postphase group received CPG-consistent antiemetic care. The prephase and postphase groups had patients who had no emesis at all, but significantly more patients in the postphase were emesis-free. Of those who had emesis, patients in the postphase group had significantly fewer days with emesis. The emesis-free plot also showed a significantly longer period until emesis in the postphase group (5 days vs 3 days; Figure 1). Of the patient- and treatment-related characteristics listed in Table 2, age was identified in a study by Dupuis and colleagues as an impacting factor of chemotherapy-induced vomiting control in pediatric patients receiving moderately or highly emetogenic chemotherapy, but not sex, cancer type, or chemotherapy emetogenicity.23 Our comparison of days of emesis between the 2 groups, adjusted for patient age, supports the conclusion of reduced emesis in the postphase group.
This study included patients with malignant and nonmalignant disorders. Anticipatory nausea and vomiting may occur in more patients with malignancy than in those with a nonmalignant disorder because of previous exposure to chemotherapy and could have affected the differences in outcomes. However, because there were proportionally more patients with a nonmalignant disorder in the prephase group, any confounding impact from anticipatory nausea and vomiting would have favored better nausea and vomiting control in the prephase group than in the postphase group. Nausea after receiving chemotherapy with or without TBI can negatively affect a patient’s QOL, but was not examined in this study because of the lack of a reliable assessment tool available at our institution. We also recognized that although the protocol implementation resulted in emesis improvement, only 27% of patients in the postphase group had complete emesis control. This low occurrence may have been limited by the patient sample size.
Updated antiemetic guidelines were published after the conclusion of this study.7,8 Palonosetron specifically is recommended in combination with dexamethasone or fosaprepitant in patients unable to receive fosaprepitant or dexamethasone, respectively. Palonosetron is also recommended in patients who are unable to receive dexamethasone plus fosaprepitant. Because of our institution’s formulary restriction, we were able to prescribe palonosetron only in patients who did not respond to ondansetron and granisetron for emesis control. On the other hand, we have modified our antiemetic protocol to add olanzapine as part of a preemptive regimen in patients aged ≥3 years who are unable to receive dexamethasone and/or aprepitant for the treatment of moderately or highly emetogenic chemotherapy because of contraindication.
Another opportunity for delivering targeted care could be the use of granisetron upfront over ondansetron based on pharmacogenetic testing. Ondansetron is extensively metabolized by several CYP450 enzymes, including CYP1A2, CYP2D6, and CYP3A4.24 The current recommendation from the Clinical Pharmacogenetics Implementation Consortium in individuals with CYP2D6 ultrarapid metabolizer phenotype is to use alternative drugs that are not predominantly metabolized by this enzyme, such as granisetron.25 In this study, only 2 patients in the postphase group switched from ondansetron to granisetron, and it was difficult to evaluate the impact on the overall emesis control. The availability of pharmacogenetic testing could provide valuable information in the initial selection of the optimal 5-HT3 antagonist for each patient.
In this study, we reported tolerance to an all-enteral antiemetic regimen and a reduction of IV antiemetics in terms of the number of doses daily. The use of the oral route is generally encouraged for medication administration because use of IV route has been associated with adverse drug events, reduced QOL, and higher cost in other studies.26-28 A reduction in the number of times a central line was accessed also aligns with our institution’s efforts to decrease central line–associated bloodstream infections.
Adequate control of nausea and vomiting allows patients to receive enteral nutrition, which is generally considered advantageous over PN because it maintains gastrointestinal tract integrity and avoids infective and metabolic complications related to PN. There were no statistical differences in PN use and the number of days to start PN between the prephase and postphase groups. Other AEs of chemotherapy with or without TBI, such as mucositis or loss of appetite because of fatigue or changes in how food tastes or smells, may have contributed to the overall use of PN, especially in patients without feeding tubes, because of contraindication or refusal. A study by Flank and colleagues reported a similar rate of PN use (83%) in children receiving HSCT conditioning, but cited a correlation of nausea and vomiting control with decreased proportion of total energy provided by PN and shorter duration of PN use.1 We did not explore these aspects, but they are favorable outcomes worthy of future investigation that would require controlling for factors, such as gut GVHD or gut infections, that necessitate the use of PN after the conditioning period.
A consideration when adopting any new guideline is balancing efficacy with cost impact. Compared with antiemetics such as ondansetron ($35.68-$41.53 for 8-mg tablet) or dexamethasone ($1.19-$1.25 for 4-mg tablet), the cost of aprepitant was significantly higher at $318.39 for a 125-mg capsule and $410.20 for suspension 125 mg/5 mL (average wholesale price or price range when there are multiple manufacturers).20 Recent studies have shown the cost-effectiveness of aprepitant in CINV prevention in adults and children receiving standard highly emetogenic chemotherapy.29,30 Although we recognized the administration savings from using fewer IV antiemetics, a potential follow-up study of cost-charge analysis would help us gain knowledge of the full financial impact of this protocol implementation in a pediatric HSCT setting.
The management of chemotherapy and radiation-induced nausea and vomiting is a high priority in the care of children undergoing HSCT. The clinical guidelines endorsed by the Children’s Oncology Group (COG) provide valuable recommendations for CINV, and adherence to these guidelines has resulted in significant improvement in CINV control.31,32 However, the application of and compliance with these guidelines remain challenging in HSCT settings because of the complex dosing and scheduling of conditioning regimens compared with those used in non-HSCT settings.33 A significant portion of patients undergoing HSCT also had previous exposure to multiple rounds of chemotherapy and therefore may have an ineffective and/or undesirable response to antiemetics. In addition, the COG-endorsed guidelines only offered a recommendation of radiation-induced nausea and vomiting in adults,31 even though TBI is a critical component of allogeneic HSCT for pediatric malignancies.34 It is therefore essential to critically assess the unique needs of each patient undergoing HSCT when devising and applying CPG-consistent antiemetic care.
Pharmacists are a critical part of the HSCT team in achieving desirable patient outcomes by ensuring medication safety and efficacy. The implementation of our antiemetic protocol relied immensely on the availability and involvement of pediatric HSCT–trained pharmacists to interview patients and families regarding previous antiemetic use, propose an antiemetic plan based on the patients’ characteristics and conditioning regimens, and closely monitor and optimize daily antiemetic use. Our protocol exemplified pharmacists’ role in the standardization and implementation of evidence-based medicine by dedicating time and effort in medication management, patient education, collaboration with the healthcare team, and quality improvement. The implementation process also revealed other opportunities for future exploration as we continue the effort to provide the best evidence-based antiemetic therapy possible, such as the use of palonosetron as recommended by CPG and the pursuit of pharmacogenetic testing availability for our patients.
Limitations
Our study had several limitations, including its retrospective design that relied on existing clinical data. Our study had a small sample size of 60 patients per group, which may have limited its ability to detect some between-group differences or generalize the findings. Only 27% of the patients in the postphase group achieved complete emesis control, suggesting that the low occurrence of complete control may have been influenced by the sample size. Also, the protocol was implemented at a single institution with a highly specialized pediatric HSCT program, including access to dedicated clinical pharmacists, which may limit the findings’ generalizability to other institutions.
Anticipatory nausea and vomiting was not specifically evaluated. This could have introduced confounding effects, because the prephase group had a higher proportion of patients with nonmalignant conditions, potentially favoring better outcomes in that group. Although this study focused on emesis control, it did not assess nausea because of the absence of a reliable assessment tool at our institution, which limits the ability to fully evaluate the impact of the intervention on patients’ QOL. Although the study showed similar rates of PN use between the prephase and postphase groups, it did not explore the correlation between improved emesis control and the proportion of total energy provided by PN or the duration of PN use. Factors such as mucositis, fatigue, or changes in taste and smell, as well as contraindications or refusal of feeding tubes, may have contributed to PN use but were not specifically analyzed.
Patients receiving posttransplant cyclophosphamide were excluded in this study to avoid overlap in emesis sources, which limits the applicability of the findings to this subset of patients who had HSCT.
This study concluded before the publication of updated antiemetic guidelines that recommend palonosetron as an alternative to ondansetron or granisetron in certain scenarios. In addition, institutional formulary restrictions limited the use of palonosetron, which may have impacted the effectiveness of antiemetic therapy in some cases. The study also did not incorporate pharmacogenetic testing, which could have informed the selection of 5-HT3 antagonists (eg, granisetron over ondansetron in CYP2D6 ultrarapid metabolizers). Without this information, the impact of genetic variability on emesis control remains unexplored.
Although this study showed a reduction in IV antiemetic drug use in the postphase group, it did not conduct a cost analysis to evaluate the financial implications of implementing the revised antiemetic protocol, including the high cost of aprepitant and the potential savings from reduced IV medication use.
Last, the inclusion of novel agents, such as olanzapine, was limited to patients aged ≥3 years because of a lack of evidence in younger children. Thus, the findings may not apply to this younger population.
These limitations highlight the need for further studies with larger sample sizes, prospective designs, and a broader scope to evaluate the full impact of pharmacist-guided, guideline-consistent antiemetic protocols on patient outcomes in pediatric HSCT settings.
Conclusion
As shown in the recent past with the development of proven and novel pharmacotherapeutics, the strategies of CINV management will likely continue to evolve. Pharmacists can play an integral role in evaluating and adapting CPG in real time, improving care for specific patients, as well as ensuring that institutional protocols are up to date. Interviewing patients and/or their families removes the trial and error often experienced when searching for an effective antiemetic regimen and empowers patients and their families to engage in their care, fostering a healthy relationship with the medical team.
Author Disclosure Statement
Dr Carpenter is a consultant for Incyte, has done research support for and is on a steering committee for Sanofi, and on the Advisory Board for Mesoblast; Dr Angus owns stock in AbbVie, Agenus, Beam Therapeutics, Crispr Therapeutics, Geron, and GSK; Dr Chan, Dr Abrass, Dr Barry, Dr Sipols, Dr Niedner, and Dr Baker have no conflicts of interest to report.
References
- Flank J, Sparavalo J, Vol H, et al. The burden of chemotherapy-induced nausea and vomiting in children receiving hematopoietic stem cell transplantation conditioning: a prospective study. Bone Marrow Transplant. 2017;52:1294-1299.
- Trigg ME, Inverso DM. Nausea and vomiting with high-dose chemotherapy and stem cell rescue therapy: a review of antiemetic regimens. Bone Marrow Transplant. 2008;42:501-506.
- Haiderali A, Menditto L, Good M, et al. Impact on daily functioning and indirect/direct costs associated with chemotherapy-induced nausea and vomiting (CINV) in a U.S. population. Support Care Cancer. 2011;19:843-851.
- Shulman DS, London WB, Guo D, et al. Incidence and causes of hospital readmission in pediatric patients after hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2015;21:913-919.
- Thorvaldson L, Remberger M, Winiarski J, et al. HLA, GVHD, and parenteral nutrition are risk factors for hepatic complications in pediatric HSCT. Pediatr Transplant. 2016;20:96-104.
- Mattsson J, Westin S, Edlund S, Remberger M. Poor oral nutrition after allogeneic stem cell transplantation correlates significantly with severe graft-versus-host disease. Bone Marrow Transplant. 2006;38:629-633.
- Hesketh PJ, Kris MG, Basch E, et al. Antiemetics: ASCO Guideline Update. J Clin Oncol. 2020;38:2782-2797. Errata in: J Clin Oncol. 2020;38:3825; J Clin Oncol. 2021;39:96
- Patel P, Robinson PD, Cohen M, et al. Prevention of acute and delayed chemotherapy-induced nausea and vomiting in pediatric cancer patients: a clinical practice guideline. Pediatr Blood Cancer. 2022;69:e30001.
- Ho VT, Soiffer RJ. The history and future of T-cell depletion as graft-versus-host disease prophylaxis for allogeneic hematopoietic stem cell transplantation. Blood. 2001;98:3192-204.
- Saad A, Taneja A, Di Stasi A, et al. Impact of high-dose steroid premedication on the outcome of myeloablative T cell replete haploidentical peripheral blood stem cell transplant. Bone Marrow Transplant. 2018;53:1345-1348.
- Patel P, Leeder JS, Piquette-Miller M, Dupuis LL. Aprepitant and fosaprepitant drug interactions: a systematic review. Br J Clin Pharmacol. 2017;83:2148-2162.
- Naik RD, V S, Singh V, et al. Olanzapine for prevention of vomiting in children and adolescents receiving highly emetogenic chemotherapy: investigator-initiated, randomized, open-label trial. J Clin Oncol. 2020;38:3785-3793.
- Flank J, Thackray J, Nielson D, et al. Olanzapine for treatment and prevention of acute chemotherapy-induced vomiting in children: a retrospective, multi-center review. Pediatr Blood Cancer. 2015;62:496-501.
- Clemmons AB, Alexander M, DeGregory K, Kennedy L. The hematopoietic cell transplant pharmacist: roles, responsibilities, and recommendations from the ASBMT Pharmacy Special Interest Group. Biol Blood Marrow Transplant. 2018;24:914-922.
- Patel P, Robinson PD, Thackray J, et al. Guideline for the prevention of acute chemotherapy-induced nausea and vomiting in pediatric cancer patients: a focused update. Pediatr Blood Cancer. 2017;64:e26542.
- Hesketh PJ, Kris MG, Basch E, et al. Antiemetics: American Society of Clinical Oncology Clinical Practice Guideline Update. J Clin Oncol. 2017;35:3240-3261.
- Paw Cho Sing E, Robinson PD, Flank J, et al. Classification of the acute emetogenicity of chemotherapy in pediatric patients: a clinical practice guideline. Pediatr Blood Cancer. 2019;66:e27646. Erratum in: Pediatr Blood Cancer. 2021;68:e28990.
- Patel P, Olteanu A, Cabral S, et al. Dexamethasone dosing for prevention of acute chemotherapy-induced vomiting in pediatric patients: a systematic review. Pediatr Blood Cancer. 2020;67:e28716.
- Emend (aprepitant) capsules, for oral use [prescribing information]. Merck & Co, Inc; May 2022. Accessed June 3, 2025. www.merck.com/product/usa/pi_circulars/e/emend/emend_pi.pdf
- Pediatric and Neonatal Lexi-Drugs. UpToDate Lexidrug online [database online]. Wolters Kluwer. Accessed June 3, 2025. https://online.lexi.com
- Bubalo J, Mulverhill K, Meyers G, et al. A randomized, placebo-controlled pilot trial of aprepitant combined with standard antiemetic therapy for the prevention of chemotherapy-induced nausea and vomiting in patients undergoing cyclophosphamide-based conditioning regimens prior to hematopoietic stem cell transplant (HSCT). Bone Marrow Transplant. 2018;53:1010-1018.
- de Jonge ME, Huitema AD, Holtkamp MJ, et al. Aprepitant inhibits cyclophosphamide bioactivation and thiotepa metabolism. Cancer Chemother Pharmacol. 2005;56:370-378.
- Dupuis LL, Tomlinson GA, Pong A, et al. Factors associated with chemotherapy-induced vomiting control in pediatric patients receiving moderately or highly emetogenic chemotherapy: a pooled analysis. J Clin Oncol. 2020;38:2499-2509.
- Dixon CM, Colthup PV, Serabjit-Singh CJ, et al. Multiple forms of cytochrome P450 are involved in the metabolism of ondansetron in humans. Drug Metab Dispos. 1995;23:1225-1230.
- Bell GC, Caudle KE, Whirl-Carrillo M, et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline for CYP2D6 genotype and use of ondansetron and tropisetron. Clin Pharmacol Ther. 2017;102:213-218.
- Kane-Gill SL, Kirisci L, Verrico MM, Rothschild JM. Analysis of risk factors for adverse drug events in critically ill patients. Crit Care Med. 2012;40:823-828.
- Westbrook JI, Rob MI, Woods A, Parry D. Errors in the administration of intravenous medications in hospital and the role of correct procedures and nurse experience. BMJ Qual Saf. 2011;20:1027-1034.
- Parker SE and Davey PG. Pharmacoeconomics of intravenous drug administration. Pharmacoeconomics. 1992;1:103-115.
- Qiu T, Men P, Sun T, Zhai S. Cost-effectiveness of aprepitant in preventing chemotherapy-induced nausea and vomiting: a systematic review of published articles. Front Public Health. 2021;9:660514.
- Sra MS, Ganguly S, Sasi A, et al. Cost-effectiveness analysis of aprepitant-based anti-emetic regimen for children receiving highly emetogenic chemotherapy: individual patient data analysis of a randomized trial. Pediatr Blood Cancer. 2022;69:e29795.
- Children’s Oncology Group. COG Supportive Care Endorsed Guidelines. Accessed March 29, 2023. www.childrensoncologygroup.org/cog-supportive-care-endorsed-guidelines
- Renaux Torres MC, Robinson PD, Sung L, et al. Outcomes of chemotherapy-induced nausea and vomiting guideline adherence in pediatric and adult patients: a systematic review. Support Care Cancer. 2024;32:455.
- Yuda S, Fuji S, Savani B, Gatwood KS. Antiemetic strategies in patients who undergo hematopoietic stem cell transplantation. Clin Hematol Int. 2022;4:89-98.
- Bunin N, Aplenc R, Kamani N, et al. Randomized trial of busulfan vs total body irradiation containing conditioning regimens for children with acute lymphoblastic leukemia: a Pediatric Blood and Marrow Transplant Consortium study. Bone Marrow Transplant. 2003;32:543-548.