Connecting Science to Practice
Lack of dosing recommendations and general avoidance of
pacritinib in patients with severe renal dysfunction (estimated
glomerular filtration rate <30 mL/min/1.73 m2) has
limited its use. The authors report safe and effective use of
reduced-dose pacritinib therapy with careful monitoring in
a patient with myelofibrosis with end-stage renal disease on
long-term hemodialysis, suggesting a safe and effective option
in these patients.
Primary myelofibrosis is a myeloproliferative neoplasm (MPN) characterized by bone marrow fibrosis, extramedullary hematopoiesis with hepatosplenomegaly, and leukoerythroblastosis in the peripheral blood.1 Patients with myelofibrosis can present with or without pancytopenia (hemoglobin <10 g/dL, platelets <50×109/L). Patients with myelofibrosis and cytopenias tend to have a poor prognosis and a more aggressive disease course.1 First-line treatment strategies for noncytopenic myelofibrosis can include hydroxyurea, the Janus kinase (JAK) 1/2 inhibitor ruxolitinib, or the JAK2 inhibitor fedratinib, which are prescribed with the goal of symptom relief and reduction of spleen size.2 The dose-limiting adverse events (AEs) of these therapies include anemia and thrombocytopenia, making these treatments challenging in patients with cytopenic myelofibrosis.2
Until the approval of pacritinib, therapeutic strategies for patients with cytopenic myelofibrosis were limited.2 Pacritinib, a selective JAK2 inhibitor, is FDA-approved for the treatment of myelofibrosis with platelets <50×109/L, because treatment with pacritinib is not associated with significant anemia or thrombocytopenia.3 This is attributed to pacritinib’s lack of effect on JAK1, the tyrosine kinase that is implicated in myelosuppression, and pacritinib’s inhibition of interleukin-1 receptor–associated kinase 1 and activin A receptor, type 1 (ACVR1)/activin receptor–like kinase 2, which reduce myelosuppression and, in the case of ACVR1, may increase hemoglobin.4-6
Pacritinib was FDA-approved at a standard dose of 200 mg twice daily based on the findings of the PAC203 study, which demonstrated higher rates of spleen volume reduction and symptomatic relief than the 100-mg twice-daily and 100-mg once-daily dosing cohorts.3,7 The current dosing guidance for pacritinib recommends the avoidance of pacritinib treatment in patients with an estimated glomerular filtration rate (eGFR) of <30 mL/min/1.73 m2 because of the potential for increased systemic exposure in this setting.3 However, chronic kidney disease (CKD) and end-stage renal disease (ESRD) have been reported in approximately 25% of all patients diagnosed with an MPN, with similar rates in all subsets of MPN.8 In one retrospective study, 29% of patients had stage 3 or 4 CKD at the time of diagnosis of MPN, with 2% of patients having stage 4 CKD (eGFR, 15-29 mL/min/1.73 m2) at the time of diagnosis.9
As a result of the clinical need to treat patients with cytopenic myelofibrosis and CKD, we report the clinical course of a patient with cytopenic myelofibrosis and concurrent ESRD who was receiving pacritinib therapy and long-term hemodialysis, and is the first patient we know to be dosed in this setting.
Case Report
We present the case of a 69-year-old man with primary cytopenic myelofibrosis and an International Prognostic Scoring System risk score of intermediate-2. His medical history was significant for hypertension and ESRD, and at the time of this report the patient was receiving hemodialysis 3 times weekly. He was initially diagnosed with CKD 3 years previously, with a baseline serum creatinine of 2.2 mg/dL and nephrotic-range proteinuria. A renal biopsy showed tubulointerstitial fibrosis with intimal fibrosis in 10 of 12 glomeruli. The patient had no immune deposits, thrombosis, thrombotic microangiopathy, or extramedullary hematopoiesis.
During this time, the patient also had splenomegaly at 20 cm, mild anemia (hemoglobin, 10.5 g/dL), leukocytosis (white blood cell count, 15×109/L), and a normal platelet count (268×109/L), which suggests his renal injury possibly resulted from his underlying MPN.10,11 No treatment or other diagnostic workup was initiated at that time at the outpatient center. Two years later, the patient had a hemoglobin level of 8.7 g/dL and a platelet count of 45×109/L. Concurrently, the patient had significant ascites and hepatosplenomegaly with a liver measurement of 20 cm and a spleen measurement of 26.5 cm in the absence of any signs of primary hepatic etiology. Ascitic fluid cytology was negative for malignancy.
A bone marrow biopsy revealed a hypercellular marrow without increased blasts and grade 3/3 fibrosis. Next-generation sequencing revealed the presence of JAK2 with a variant allele frequency of 59.6% and 2 ASXL1 mutations (variant allele frequency, 3.9% and 4.9%), which is consistent with primary myelofibrosis. As a result of the concurrent cytopenias, ruxolitinib therapy was contraindicated and the patient was instead started on treatment with pacritinib at an empirically reduced dose of 100 mg daily instead of the standard dose.7,12,13 At the time, the patient’s serum creatinine was 4.3 mg/dL. He was not receiving any CYP3A4-modulating therapies that interact with pacritinib, and his hepatic function was normal.
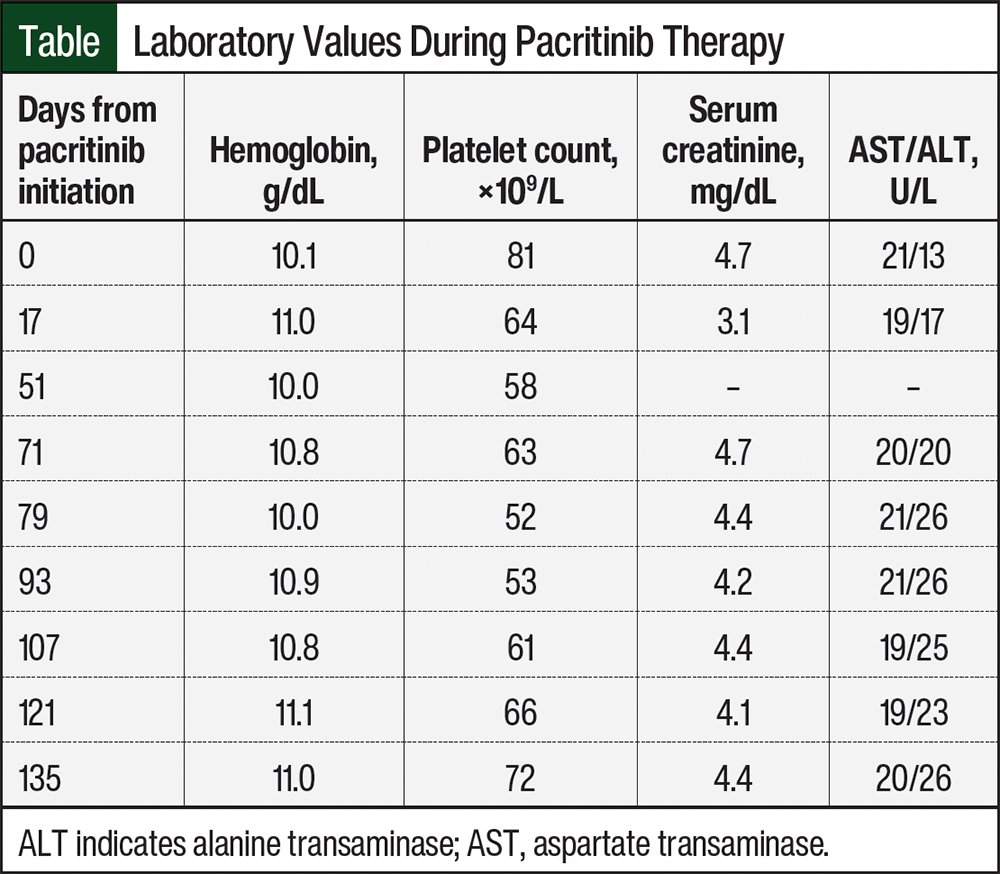
Over the next 16 weeks, the patient’s hemoglobin level improved from 9.4 g/dL to 11.1 g/dL, and his platelet count remained stable (Table). In the absence of any apparent AEs, his dose of pacritinib was increased from 100 mg daily to 100 mg twice daily. Eight weeks later, the patient’s hemoglobin and platelet counts remained stable, at 10.8 g/dL and 61×109/L, respectively, in the absence of transfusion, and his dose of pacritinib was further increased to 200 mg in the morning and 100 mg in the evening. No AEs were reported on dose escalation, and routine electrocardiogram monitoring showed normal QTc intervals. A repeat splenic ultrasound performed 5 months from the start of the patient’s pacritinib therapy demonstrated a reduction in splenic size from 26 cm to 21 cm. He continues to remain stable at the time of this writing.
Discussion
MPN-related nephropathy is poorly defined.14 Lucijanic and colleagues reported CKD in 26.1% of patients with MPN, with higher rates recorded in patients with cardiovascular comorbidities, with longstanding MPN, or who initially presented with stronger features of myeloproliferation.8 In a later study by these same investigators, the kidney biopsies of patients with MPN who did not previously have glomerular pathologies at baseline showed increased rates of glomerular hypercellularity and mesangial sclerosis, with some patients demonstrating evidence of renal extramedullary hematopoiesis.11 Another study of 29 patients with MPN showed that 11% to 29% of patients have a concurrent diagnosis of stage 3 or 4 CKD at the time of MPN diagnosis, and approximately 20% of patients with MPN have a rapid rate of eGFR decline that exceeds the expected trajectory of age-related renal function changes.15 This same study also reported renal histologic findings of segmental and global glomerulosclerosis and extramedullary hematopoiesis in 66% and 17% of patients with MPN, respectively.15
Renal impairment is also seen in patients with acute or chronic myelomonocytic leukemia and is likely caused by monocytic infiltration; a similar process mediated by increased monocytes may contribute to the pathology of renal disease in patients with MPN as well.16 Currently, kidney biopsies are not frequently performed in patients with MPN, especially those with cytopenias, because of an increased risk for bleeding. However, this prevalence of renal insufficiency in patients with MPN warrants efforts to enable patient access to as many active agents as possible. As of the time of this writing, the NCCN’s treatment guidelines do not provide guidance on the management of patients with MPN and concurrent advanced-stage CKD or ESRD.17
Although pacritinib is predominantly metabolized hepatically via CYP3A4, 6% of pacritinib’s parent drug was detected in the urine in initial pharmacokinetic studies, indicating some degree of renal excretion.3 The current recommendation to avoid treatment with pacritinib in patients with an eGFR of <30 mL/min/1.73 m2 is based on pharmacokinetic studies that demonstrate a clinically significant increase in pacritinib exposure compared with cohorts with normal renal function.3 There was an approximate 30% increase in Cmax and area under the curve of pacritinib in patients with an eGFR of 15 to 29 mL/min/1.73 m2 and an eGFR of <15 mL/min/1.73 m2 who are undergoing hemodialysis compared with patients with an eGFR of ≥90 mL/min/1.73 m2 after the administration of a single dose of 400 mg of pacritinib.3 It is unclear if these pharmacokinetic parameter changes would still be observed to this degree with a lower pacritinib dose of 100 to 200 mg, like we administered to our patient.
Considering the impact of renal dysfunction on pacritinib’s pharmacokinetics, the phase 3 PERSIST-1 and PERSIST-2 trials evaluated the efficacy of pacritinib in patients with myelofibrosis, excluding patients with a serum creatinine >2.5 mg/dL; hence, there are no data demonstrating the safe use of pacritinib in this patient population.12,13 Based on our experience with this patient, providers who manage similar patients with myelofibrosis and ESRD may consider an initial starting dose of 100 mg daily and escalate the dose in 100-mg increments every 4 weeks in the absence of AEs. We did not escalate dosing beyond 200 mg in the morning and 100 mg in the evening, so the safety of a standard 200-mg twice-daily dose in this patient population is unknown. Based on our patient’s experience, renal insufficiency should not prevent treatment with pacritinib at reduced doses in otherwise appropriate candidates with close monitoring. Even with prolonged dosing in patients with a normal glomerular filtration rate and severe baseline thrombocytopenia, there were no cases of excess bleeding, cardiac AEs, secondary malignancy, or venous thromboembolism in patients receiving long-term pacritinib therapy, which strengthens the argument for its safety.18
Conclusion
To date, there are no dose recommendations for pacritinib in the setting of renal dysfunction, and the avoidance of treatment with pacritinib is recommended in patients with an eGFR of <30 mL/min/1.73 m2.
We demonstrated successful treatment with reduced-dose pacritinib, with positive efficacy outcomes and a tolerable safety profile, in a patient with myelofibrosis and ESRD who was receiving hemodialysis. Additional data are warranted at this time to further elucidate the ideal dosing of pacritinib in this unique patient population.
Dr Ulrickson is a consultant for Abbvie, BMS, and Genentech; Dr Roach, Dr Heers, Dr Dave, and Dr Pemmaraju have no conflicts of interest to report.
References
- Benites BD, Costa Lima CS, Lorand-Metze I, et al. Primary myelofibrosis: risk stratification by IPSS identifies patients with poor clinical outcome. Clinics (Sao Paulo). 2013; 68:339-343.
- Tefferi A. Primary myelofibrosis: 2021 update on diagnosis, risk-stratification and management. Am J Hematol. 2021;96:145-162.
- Vonjo (pacritinib) capsules, for oral use [prescribing information]. CTI BioPharma Corp; November 2024. Accessed July 9, 2025. www.accessdata.fda.gov/drugsatfda_docs/label/2024/208712s003lbl.pdf
- Reynolds SB, Pettit K. New approaches to tackle cytopenic myelofibrosis. Hematology Am Soc Hematol Edu Program. 2022;2022:235-244.
- Singer JW, Fleishman A, Al-Fayoumi S, et al. Inhibition of interleukin-1 receptor-associated kinase 1 (IRAK1) as a therapeutic strategy. Oncotarget. 2018;9:33416-33439.
- Oh S, Mesa R, Harrison C, et al. MPN-145 retrospective analysis of anemia benefit of pacritinib from the PERSIST-2 trial. Clin Lymphoma Myeloma Leuk. 2022;22(suppl 2):S327.
- Gerds AT, Savona MR, Scott BL, et al. Determining the recommended dose of pacritinib: results from the PAC203 dose-finding trial in advanced myelofibrosis. Blood Adv. 2020;4:5825-5835.
- Lucijanic M, Galusic D, Krecak I, et al. Reduced renal function strongly affects survival and thrombosis in patients with myelofibrosis. Ann Hematol. 2020;99:2779-2785.
- Christensen AS, Moller JB, Hasselbalch HC. Chronic kidney disease in patients with the Philadelphia-negative chronic myeloproliferative neoplasms. Leuk Res. 2014;38:490-495.
- Philipponnet C, Ronco P, Aniort J, et al. Membranous nephropathy and intrarenal extramedullary hematopoiesis in a patient with myelofibrosis. Am J Kidney Dis. 2017;70:874-877.
- Lucijanic M, Krecak I, Kusec R. Renal disease associated with chronic myeloproliferative neoplasms. Expert Rev Hematol. 2022;15:93-96.
- Mesa RA, Vannucchi AM, Mead A, et al. Pacritinib versus best available therapy for the treatment of myelofibrosis irrespective of baseline cytopenias (PERSIST-1): an international, randomised, phase 3 trial. Lancet Haematol. 2017;4:e225-e236.
- Mascarenhas J, Hoffman R, Talpaz M, et al. Pacritinib vs best available therapy, including ruxolitinib, in patients with myelofibrosis: a randomized clinical trial. JAMA Oncol. 2018;4:652-659.
- Del Sordo R, Brugnano R, Covarelli C, et al. Nephrotic syndrome in primary myelofibrosis with renal extramedullary hematopoiesis and glomerulopathy in the JAK inhibitor era. Clin Nephrol Case Stud. 2017;5:70-77.
- Büttner-Herold M, Sticht C, Wiech T, et al. Renal disease associated with myeloproliferative neoplasms and myelodysplastic syndrome/myeloproliferative neoplasms. Histopathology. 2021;78:738-748.
- Tefferi A, Shah S, Mudireddy M, et al. Monocytosis is a powerful and independent predictor of inferior survival in primary myelofibrosis. Br J Haematol. 2018;183:835-838.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): myeloproliferative neoplasms. Version 1.2025. Accessed July 9, 2025. www.nccn.org/professionals/physician_gls/pdf/mpn.pdf
- Pemmaraju N, Harrison C, Gupta V, et al. Risk-adjusted safety analysis of the oral JAK2/IRAK1 inhibitor pacritinib in patients with myelofibrosis. EJHaem. 2022;3:1346-1351.