Connecting Science to Practice
This study sought to determine whether differences in dose
modifications were seen due to poly (ADP-ribose) polymerase
(PARP) inhibitor adverse events (AEs) between patients
harboring germline and somatic homologous recombination
deficiency (HRD) mutations. Differences in AE rates
are not clearly established in the literature, and this research
advances the practice of hematology/oncology pharmacy by
providing real-world data regarding safety and efficacy of
PARP inhibitors. Patient outcomes will be improved with a
better understanding of which populations may benefit the
most from PARP inhibitor treatment and which characteristics
are associated with increased efficacy. Whereas the incidence
of PARP inhibitor–related AEs was not significantly
different among germline and somatic HRD mutations,
6-month progression-free survival was significantly higher in
the germline group, which could be attributed to a higher
number of gynecologic malignancies and a higher number of
patients with BRCA1/2 mutations.
Poly (ADP-ribose) polymerase (PARP) inhibitors are often used for the treatment of cancers with homologous recombination deficiency (HRD). HRD is characterized by the inability of a cell to effectively repair DNA double-strand breaks using the homologous recombination repair (HRR) pathway.1 The BRCA1 and BRCA2 genes have an established role in the HRR pathway in maintaining genome integrity by repairing double-strand DNA breaks. Other genes, such as ATM, PALB2, RAD51, and CHEK2, also have a role in the HRR pathway via similar mechanisms.1 PARP includes 17 proteins involved in cellular processes, such as the stress response, chromatin remodeling, and DNA repair and apoptosis.2 PARP inhibitors block PARP enzymes involved in DNA transcription, cell cycle regulation, and DNA repair.2 PARP detects single-stranded DNA breaks and promotes base excision repair, which prevents double-stranded DNA breaks from occurring.2 PARP inhibitors also induce synthetic lethality in HRD mutations through the formation of double-stranded DNA breaks, which leads to disruption of cellular homeostasis and cell death.2 PARP inhibitors are approved for patients with HRD mutations in gynecologic, breast, prostate, and pancreatic cancers.3,4
The efficacy of PARP inhibitors between germline versus somatic HRD has been evaluated in a meta-analysis by Mohyuddin and colleagues that indicated similar response rates of PARP inhibitor therapy in patients with germline and somatic BRCA1/2 mutations.5 Adolphsen and colleagues determined the time to next treatment after PARP inhibitor therapy for ovarian cancer was not significantly different between patients with germline versus somatic HRD.6 In addition, Batalini and colleagues investigated germline BRCA1/2 mutations versus somatic BRCA1/2 mutations and germline PALB2 mutations in breast cancer and concluded a similar benefit from PARP inhibitors.7 PARP inhibitor adverse event (AE) differences among germline versus somatic HRD mutations are not well established in the literature. Homologous recombination genes have higher levels of HRD proteins and genes through the myeloid cell lineage and tissues, suggesting that patients with germline mutations may have more AEs compared with patients with somatic mutations.8
The most common AEs associated with PARP inhibitors are anemia, neutropenia, thrombocytopenia, and fatigue.9 PARP inhibitors also carry a risk of secondary hematologic malignancies, such as acute myeloid leukemia and myelodysplastic syndrome.9 Permanent discontinuation of PARP inhibitor therapy is recommended if secondary hematologic malignancy is confirmed or if a patient develops pneumonitis secondary to a PARP inhibitor.9 The most common grade 3 or 4 AE is anemia, which usually improves after dose reductions.9-11 Dose holding until recovery is recommended for grade 4 neutropenia, grade 3 or 4 thrombocytopenia, and prolonged hematologic dysfunction. Dose reduction is recommended for grade ≥3 anemia, grade 4 neutropenia, grade 3 or 4 thrombocytopenia, other prolonged hematologic dysfunction, and gastrointestinal AEs resulting in performance status reduction.9 The purpose of this study was to determine whether differences were seen in dose modifications due to PARP inhibitor AEs between patients harboring germline versus somatic HRD mutations, given the paucity of published literature on this topic.
Methods
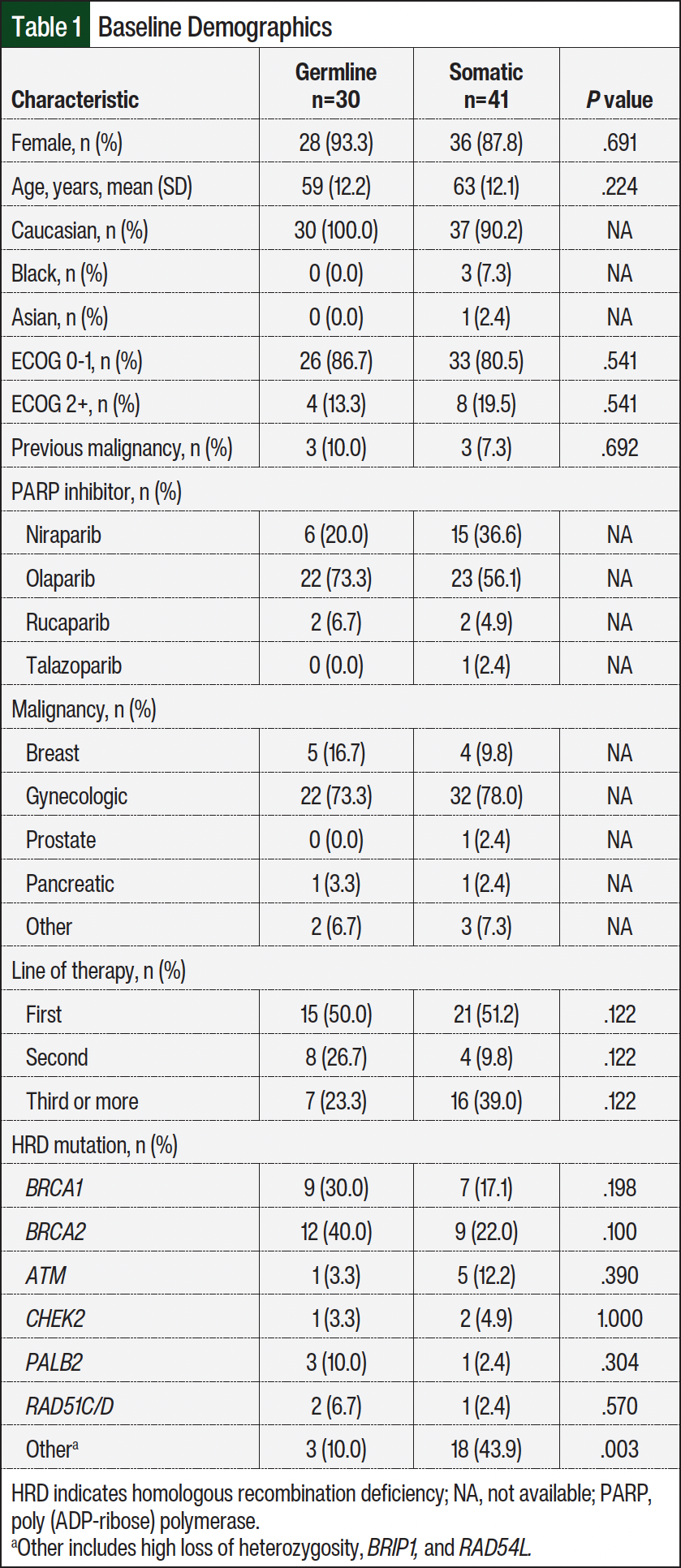
This was a retrospective cohort study of PARP inhibitor utilization at University of Kentucky Markey Cancer Center from June 2021 to July 2023. Patients were included if they were ≥18 years, treated with a PARP inhibitor during the study period, and had completed germline and somatic genetic testing. Patients were excluded if treatment with a PARP inhibitor was a part of a research study, or if the patient did not begin prescribed treatment. HRD mutations included in the study were BRCA1, BRCA2, ATM, CHEK2, PALB2, RAD51C, RAD51D, and others, such as high loss of heterozygosity (LOH), BRIP1, and RAD54L. High LOH was confined to the somatic group. Somatic mutations were defined as mutations detected in the tumor sample that were not detected in the germline sample. Germline mutations were classified as those detected in the germline sample. Ambry Genetics, Myriad Genetics, Invitae, and Quest Diagnostics were used for germline testing. Somatic testing was performed before beginning PARP inhibitor treatment. Baseline demographic characteristics are shown in Table 1. The primary end point was a composite of the frequency of dose adjustment, discontinuation, or holding due to AEs. Secondary end points were 6-month progression-free survival (PFS); 12-month overall survival (OS); frequency of secondary malignancies; AEs that led to dose adjustment, discontinuation, or hold; and 6-month PFS in BRCA1 or BRCA2 mutation carriers.
Data were collected via REDCap data collection system. Categorical outcomes were analyzed using Pearson’s chi-square test or Fisher’s exact test as appropriate and reported as counts and percentages. Continuous outcomes were analyzed using the Student’s t test and reported as means and standard deviations. All bivariate analyses were performed using IBM SPSS Statistics 29.0. Variables found to be significant in the bivariate analysis were carried forward into a multivariable logistic regression to model mortality using a backward elimination variable selection criterion with SAS 9.4. All statistical analyses used an alpha level of 0.05.
Results
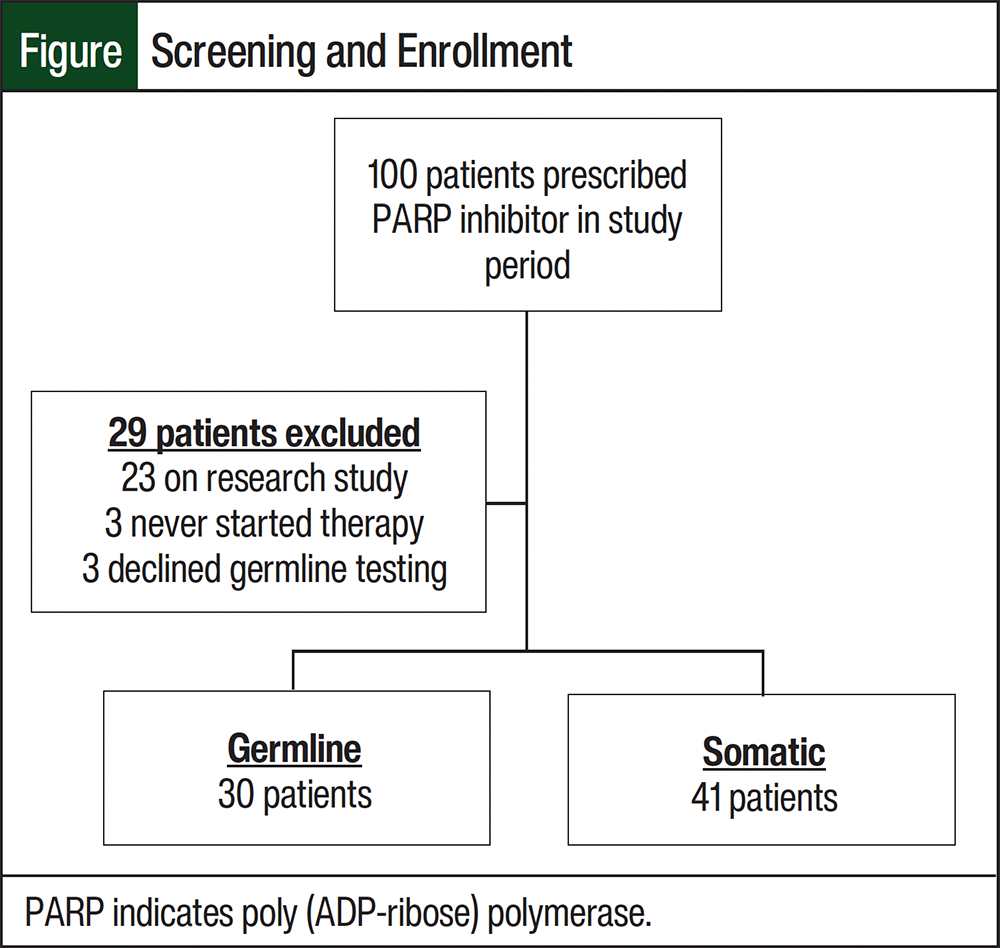
A total of 100 patients who had received a PARP inhibitor during the study period were analyzed. In all, 2 patients were excluded from the study—23 patients who received a PARP inhibitor as part of a research study, 3 who never started the prescribed therapy, and 3 who declined germline genetic testing. The final analysis included 71 patients: 30 patients who had a germline mutation and 41 who had a somatic mutation not identified in the germline (Figure). Of the 30 patients with germline mutations, all had either the same mutation confirmed, as detected in somatic testing, or were presumed positive in the somatic report from Ambry Genetics. Of the 30 patients with germline mutations, 24 were tested through Ambry, 3 through Invitae, 1 through Myriad, 1 through Quest, and 1 unknown due to testing in 2011.
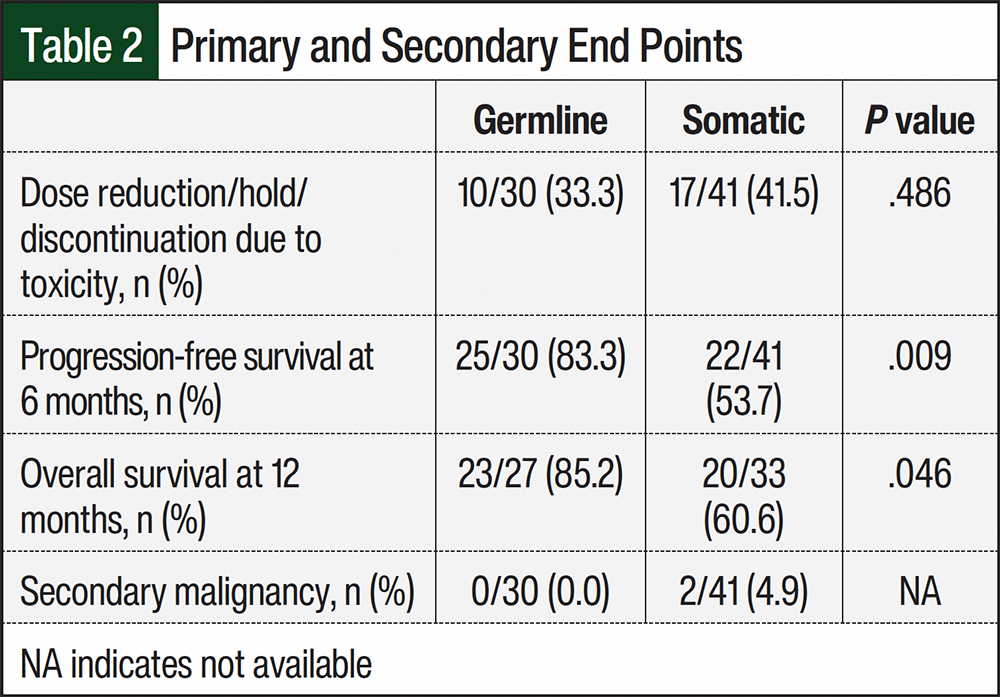
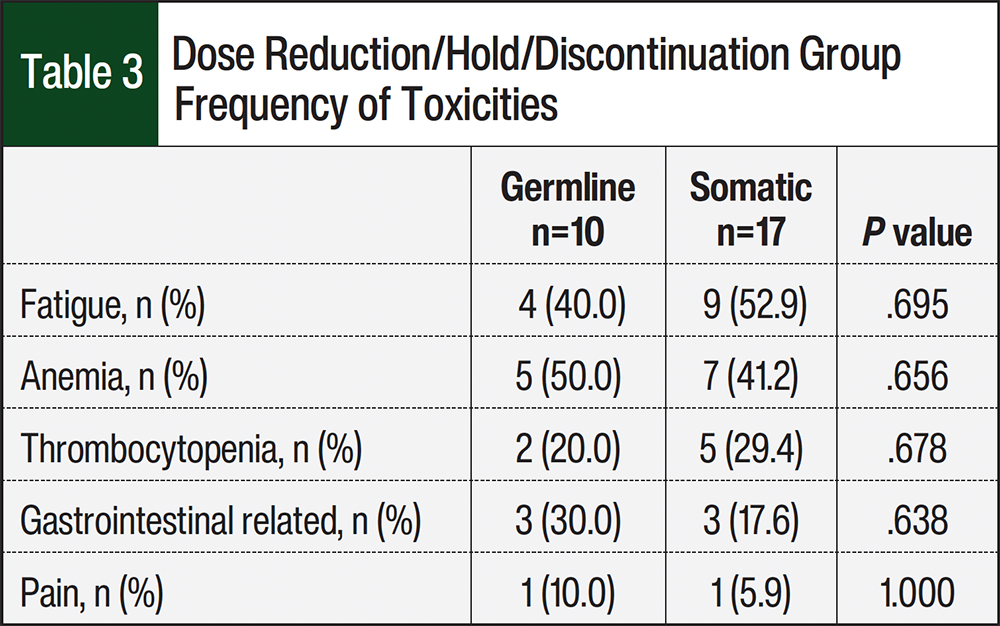
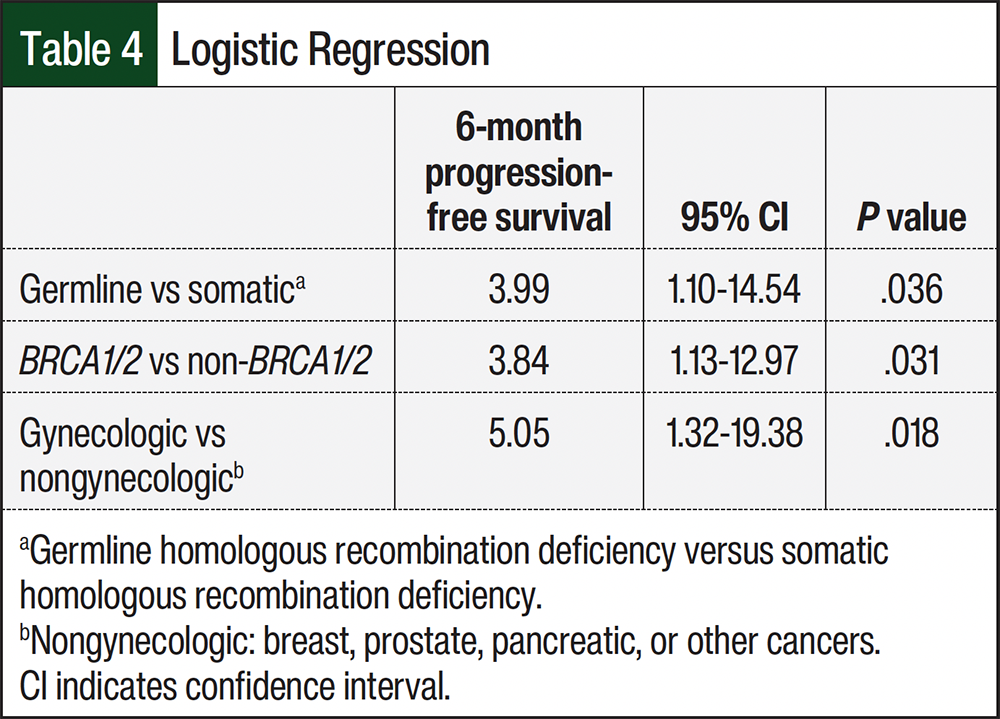
The incidence of dose reduction, hold, or discontinuation due to AEs was 33.3% in the germline group versus 41.5% in the somatic group (P=.486; Table 2). The most common AE that led to dose reduction, hold, or discontinuation was fatigue, followed by anemia, thrombocytopenia, gastrointestinal-related AEs, and pain (Table 3). PFS at 6 months was 83.3% in the germline group versus 53.7% in the somatic group (P=.009). OS at 12 months was 85.2% in the germline group versus 60.6% in the somatic group (P=.046; Table 2). The final multivariable logistic model included the following 3 predictors: germline versus somatic, BRCA1/2 versus non-BRCA1/2 HRD mutations, and gynecologic versus other malignancies. PFS at 6 months was more likely for patients with germline mutations, BRCA1/2 mutations, and gynecologic malignancy. The odds of 6-month PFS were 3.99 times higher for the germline than somatic group (95% confidence interval [CI], 1.10-14.54), 3.84 times higher in the BRCA1/2 group than non-BRCA1/2 group (95% CI, 1.13-12.97), and 5.05 times higher in patients with gynecologic malignancies than nongynecologic malignancies (95% CI, 1.32-19.38; Table 4). Two patients had presumed secondary malignancies from PARP inhibitor treatment with acute myeloid leukemia and myelodysplastic syndrome during the study period, and both patients had somatic mutations.
Discussion
No significant difference was seen in PARP inhibitor dose-limiting AEs between patients with germline and somatic HRD mutations. The rate of dose reduction, hold, or discontinuation was 33.3% to 41.5%, which is similar to the rate seen in the literature, with dose reductions of 28% to 53%.10,11 The most common dose-limiting AEs were anemia and fatigue, which is similar to previous reports.4-6,11 Dhawan and colleagues found a significant difference in neutrophil decrease in germline carriers compared with nongermline carriers when treated with carboplatin and talazoparib (78% vs 63% decrease, P<.001). Platelet decrease was predicted to be significantly larger in germline BRCA carriers than noncarriers based on a pharmacokinetic safety model.8 The proposed mechanism for increased hematologic AEs in germline carriers is increased susceptibility of hematopoietic cells that harbor a germline defect in DNA repair.8
In our study, 6-month PFS and 12-month OS were improved in patients with germline mutations versus somatic mutations. This conflicts with previous reports, which found no difference in mortality between germline and somatic mutations.5,7 However, there was a higher incidence of ≥3 lines of therapy in the somatic group; although this did not meet clinical significance, it could contribute to our findings. The lower 6-month PFS and 12-month OS in the somatic group could be attributed to later lines of therapy potentially having a detrimental effect on PFS and OS. The OReO/ENGOT-ov38 study investigated the use of maintenance olaparib rechallenge, and the patients with a greater number of previous regimens had a nonsignificant decrease in PFS in the subgroup analysis.12 Furthermore, there were more BRCA1/2 mutations in the germline group, which previous studies have shown increased the efficacy of PARP inhibitor therapy in BRCA1/2 mutations compared with other HRD mutations.6,10,13 The TALAPRO-2 study showed significant improvement in PFS in the patients receiving PARP inhibitor treatment for BRCA1/2 mutations (P<.001), whereas the incidence of PFS in the non-BRCA1/2 subgroup was not significant (P=.120).10 Olaparib’s approval for ovarian cancer was based on the SOLO-1 trial, which only included patients with BRCA1/2 mutations.11 This study showed a 70% lower risk of disease progression or death with maintenance olaparib in newly diagnosed advanced ovarian cancer and a BRCA1/2 mutation.11 The PAOLA-1/ENGOT-ov25 trial showed a clinically meaningful benefit in OS and PFS in both BRCA1/2 and non-BRCA1/2 HRD mutations in newly diagnosed ovarian cancer, but the subgroup analysis showed median PFS was double in the BRCA1/2 group versus non-BRCA1/2 group (60.7 months vs 30.0 months).13 This study showed increased efficacy of PARP inhibitor therapy in patients with BRCA1/2 HRD mutations, which is consistent with subgroup analyses in the literature.6,10,13
The majority of patients who received a PARP inhibitor during the study period and met inclusion criteria had a gynecologic malignancy, which is in line with the FDA-approved indications for PARP inhibitors.9,14-16 Patients who received a PARP inhibitor for a gynecologic malignancy had improved PFS compared with the other cancer types. However, the number of subjects with nongynecologic malignancy in both groups was low, which was a limitation in our study. The results of this study can be best applied to patients with gynecologic malignancies with BRCA1/2 mutations. In breast cancer, PARP inhibitors are approved only for germline BRCA1/2 or HRD mutations and not somatic HRD mutations.9,16 PARP inhibitors may be more effective in gynecologic malignancies because gynecologic malignancies, ovarian cancer in particular, harbor a high frequency of HRD genomic background.17 This study supports the use of PARP inhibitors in gynecologic malignancies for FDA-approved indications for both germline and somatic HRD mutations.9,14,15
Study Limitations
Strengths of this study include the study design and ability to report specific AEs stemming from treatment with PARP inhibitors. Limitations of this study include the small sample size. This was a single-center study, so the population may not translate to the general population. The 12-month OS data were premature, because 11 of the 71 patients had begun PARP inhibitor treatment within 1 year of data collection.
Conclusion
In this study, the incidence of AEs in patients receiving a PARP inhibitor that warranted a dose modification was not significantly different among germline and somatic HRD mutations. PFS at 6 months in the germline group was significantly higher than the somatic group. In addition, 6-month PFS was significantly higher for patients with gynecologic malignancies than nongynecologic malignancies and for patients with BRCA1/2 mutations versus other HRD mutations. Improved PFS in the germline group was likely driven by a higher number of BRCA1/2 mutations in the germline group.
Author Disclosure Statement
The authors have no disclosures, and no funding was received in relation to this study.
References
- Heeke AL, Pishvaian MJ, Lynce F, et al. Prevalence of homologous recombination-related gene mutations across multiple cancer types. JCO Precis Oncol. 2018:2018:PO.17.00286. doi:10.1200/PO.17.00286
- Rose M, Burgess JT, O’Byrne K, Richard DJ. PARP inhibitors: clinical relevance, mechanism of action and tumor resistance. Front Cell Dev Biol. 2020;8:564601. doi: 10.3389/fcell.2020.564601
- Stewart MD, Merino Vega D, Arend RC, et al. Homologous recombination deficiency: concepts, definitions, and assays. Oncologist. 2022;27:167-174. doi:10.1093/oncolo/oyab053
- Lee M, Pant S. Personalizing medicine with germline and somatic sequencing in advanced pancreatic cancer: current treatments and novel opportunities. ASCO Educational Book. 2021:41:e153-e165. doi:https://doi.org/10.1200/EDBK_321255
- Mohyuddin GR, Aziz M, Britt A, et al. Similar response rates and survival with PARP inhibitors for patients with solid tumors harboring somatic versus germline BRCA mutations: a meta-analysis and systematic review. BMC Cancer. 2020:20:507. doi:10.1186/s12885-020-06948-5
- Adolphsen J, Monson T, Martin G, et al. Duration of response to PARP inhibitors for maintenance treatment of ovarian cancer in patients with germline or somatic HRD. J Hematol Oncol Pharm. 2023;13:192-198.
- Batalini F, Madison RW, Sokol ES, et al. Homologous recombination deficiency landscape of breast cancers and real-world effectiveness of poly ADP-ribose polymerase inhibitors in patients with somatic BRCA1/2, germline PALB2, or homologous recombination deficiency signature. JCO Precis Oncol. 2023;7:e2300091. doi:10.1200/PO.23.00091
- Dhawan MS, Bartelink IH, Aggarwal RR, et al. Differential toxicity in patients with and without DNA repair mutations: phase I study of carboplatin and talazoparib in advanced solid tumors. Clin Cancer Res. 2017;23:6400-6410. doi:10.1158/1078-0432.CCR-17-0703
- Lynparza [prescribing information]. AstraZeneca; 2025. Accessed March 5, 2026. www.lynparzahcp.com
- Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): a randomised, placebo-controlled, phase 3 trial. Lancet. 2023;402: 291-303. doi:10.1016/S0140-6736(23)01055-3
- Moore K, Colombo N, Scambia G, et al. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer. N Engl J Med. 2018;379:2495-2505. doi:10.1056/NEJMoa1810858
- Pujade-Lauraine F, Selle G, Scambia G, et al. Maintenance olaparib rechallenge in patients with platinum-sensitive relapsed ovarian cancer previously treated with a PARP inhibitor (OReO/ENGOT-ov38): a phase IIIb trial. Ann Oncol. 2023;34:1152-1164. https://doi.org/10.1016/j.annonc.2023.09.3110
- Ray-Coquard I, Leary A, Pignata S, et al. Olaparib plus bevacizumab first-line maintenance in ovarian cancer: final overall survival results from the PAOLA-1/ENGOT-ov25 trial. Ann Oncol. 2023;34:681-692. https://doi.org/10.1016/j.annonc.2023.05.005
- Zejula [prescribing information]. GlaxoSmithKline; 2025. Accessed March 15, 2026. zejula-tablets-pi-oil.pdf
- Rubraca [prescribing information]. Tolmar; 2025. Accessed March 15, 2026. RubracaUSPI.pdf
- Talazoparib [prescribing information]. Pfizer; 2025. Accessed March 13, 2026. labeling.pfizer.com/ShowLabeling.aspx?id=20582
- Li T, Wang X, Qin S, et al. Targeting PARP for the optimal immunotherapy efficiency in gynecologic malignancies. Biomed Pharmacother. 2023;162:114712. doi:10.1016/j.biopha.2023.114712