Connecting Science to Practice
Cardio-oncology is an emergent field that is rapidly evolving
with continued FDA approvals of new therapies that
can cause cardiovascular adverse events (AEs). Within this
context, it would be helpful to better understand educational
needs and management patterns among different
types of healthcare providers, such as pharmacists, advanced
practice providers, and physicians. A 15-question
survey was distributed to healthcare providers who assessed
cancer therapy–related cardiovascular AEs and associated
drug interactions to identify gaps in clinical practice. This
survey demonstrated that topics including immune checkpoint
inhibitor–associated myocarditis, immune modulator–associated thrombosis/thrombotic events, Bruton tyrosine
kinase inhibitor–associated bleeding, and atrial
fibrillation showed the highest educational needs. Furthermore,
survey results provided evidence of the importance
of short-term needs for specific topics and the concept of
more structured training for all healthcare providers who
manage these patients, including pharmacists.
The accelerated approval of novel oncolytic agents has made numerous pivotal therapies available to substantially improve the outcomes of several cancer types.1 The real-world use of select therapies has increased the awareness of cancer therapy–related cardiovascular toxicities (CTR-CVTs), with the first comprehensive guidelines specific to CTR-CVTs being published by the European Society of Cardiology in 2022.2 Before these guidelines were published, guidance from various medical organizations routinely focused on a specific population (eg, childhood cancer survivors) or type of cancer or cardiac toxicity (anthracycline use in breast cancer).3-5 With cardio-oncology emerging as a well-recognized interdisciplinary field, identifying the targeted education of healthcare providers (HCPs) who manage patients with CTR-CVTs is warranted.
In 2015, Sulpher and colleagues conducted a 2-part, email-based survey of HCPs who manage cardiac disease in patients with cancer.6 The survey yielded 393 responses, and the results revealed differing opinions between cardiologists and oncologists regarding a formal definition of cardiotoxicity and the diagnosis, management, and monitoring of CTR-CVTs.6 In 2019, Peng and colleagues published the results of a 45-question survey completed by cardiologists, oncologists, and other providers (such as cardio-oncologists, pediatric oncologists, radiation oncologists, nurse practitioners, and pharmacists, among others).7 This survey yielded 160 responses, and the results again demonstrated a disconnect between cardiologists and oncologists regarding the prevention of and treatment strategies for CTR-CVTs.7 Although these surveys demonstrate a disconnect between cardiologists and oncologists in various aspects of CTR-CVT management, perceived educational needs were not addressed.
To gain a better understanding of knowledge gaps in cardio-oncology, the Pharmacy Workgroup of the International Cardio-Oncology Society (IC-OS) conducted a 16-question survey distributed to HCPs in cardio-oncology from multiple disciplines and specialties (Appendix). The survey was distributed using email listservs of targeted professional pharmacy and multidisciplinary organizations with a specialization in cardio-oncology, cardiology, or hematology/oncology (eg, the IC-OS, Hematology/Oncology Pharmacy Association, American College of Clinical Pharmacy, and American Society of Health-System Pharmacists). The survey assessed background (eg, training, setting), the frequency of CTR-CVTs managed, the providers’ comfort in managing CTR-CVTs, and preferences for future educational topics (Appendix). The survey questions were identical for all disciplines, except for degree/training. The survey was maintained through Google Forms, and the responses were collected over two 4- to 8-week time frames. All responses were analyzed via descriptive methods in aggregate and with comparisons based on background training (physician, pharmacist, other provider) and specialty training (cardiology, hematology/oncology).
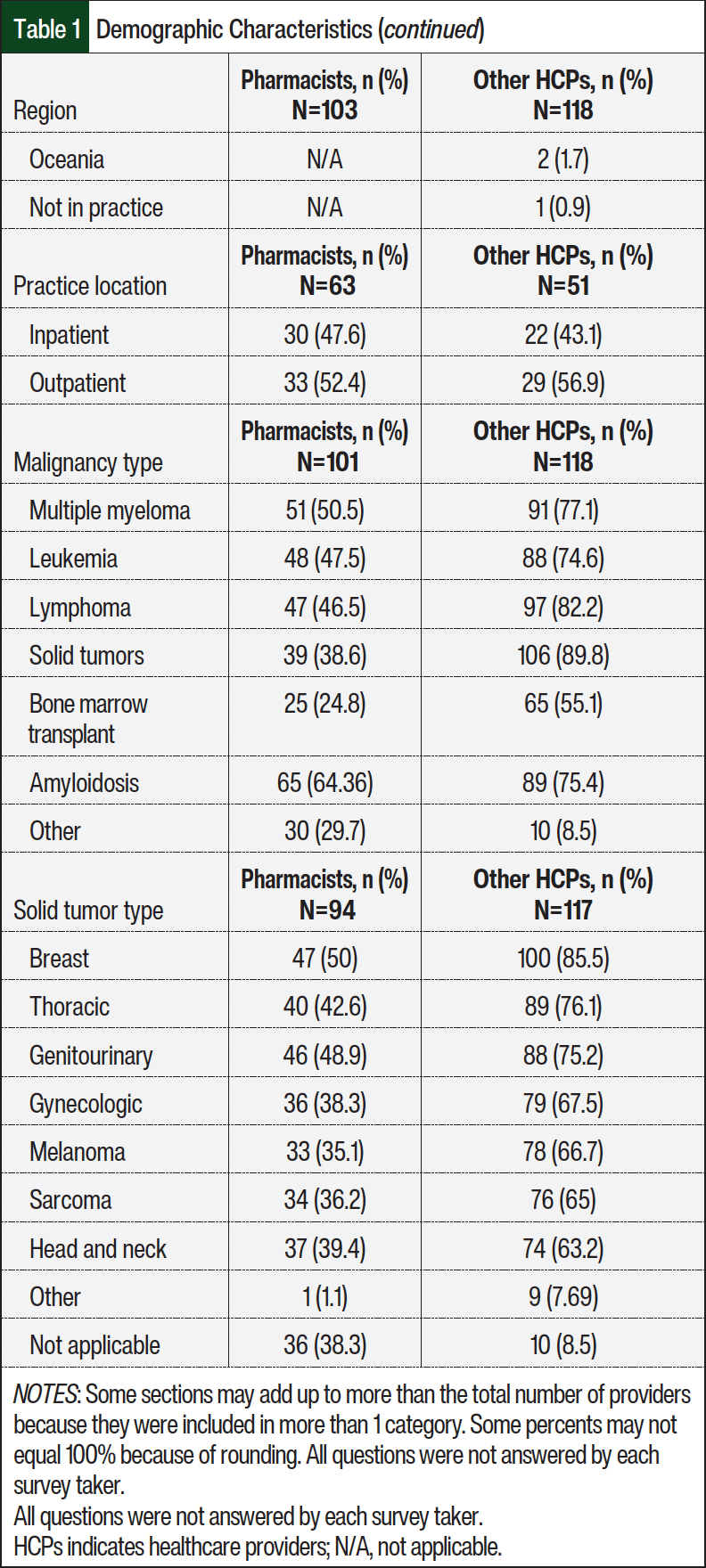
Of the 220 survey respondents, approximately 46% were pharmacists and 54% were other HCPs (>80% physicians; Table 1). The respondents predominately practiced in North America (59%) and Europe (20%), with most at academic medical centers (65%, academic; 35%, community) and primarily specialized in cardiology (71% cardiology, 24% oncology, 14% hematology). Cardiology and hematology/oncology HCPs included all disciplines within the specialty area (eg, physicians, pharmacists, other providers). Overall, the HCPs reported that the types of malignancies managed in their practice were primarily solid tumors (65%); however, malignant hematology management was also common (>60%; Table 1).

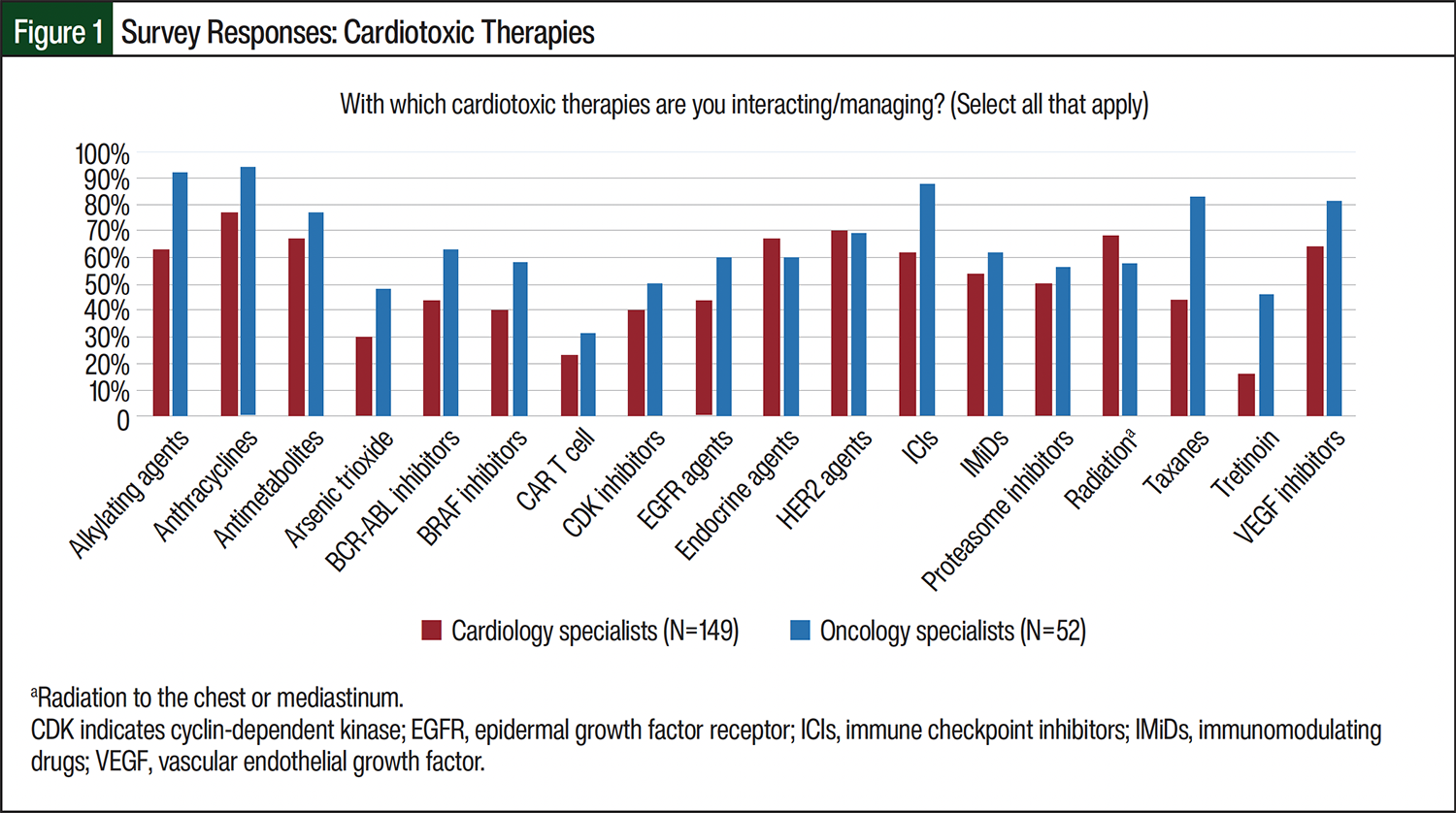
When asked “With which cardiotoxic therapies are you interacting/managing?,” more than 50% of the providers answered anthracyclines (93%), alkylating agents (78%), immune checkpoint inhibitors (76%), and vascular endothelial growth factor (VEGF) inhibitors (77%; Figure 1). When asked “Which of the following CTR-CVTs do you often see/manage?,” all of the HCPs (n=220) reported that cancer therapy–related cardiac dysfunction (CTRCD) was the most frequent CTR-CVT managed (88%), although CTRCD was more frequently managed by cardiology HCPs (95%, n=157) than by hematology/oncology HCPs (78%, n=87; Figure 2). Although cardiology HCPs reported managing atrial fibrillation (AF)/atrial flutter, coronary artery disease, coronary vasospasm, and valvular disease more often, hematology/oncology HCPs reported more frequently managing bleeding, QT prolongation/torsades de pointes, and venous thromboembolism. Pharmacists (n=102) and nonpharmacist HCPs (n=118) reported frequently managing CTRCD (77% and 97%, respectively). Overall, pharmacists reported managing all CTR-CVTs less often than nonpharmacist HCPs, especially AF/flutter, coronary artery disease/coronary vasospasm, and bradycardia/atrioventricular block.
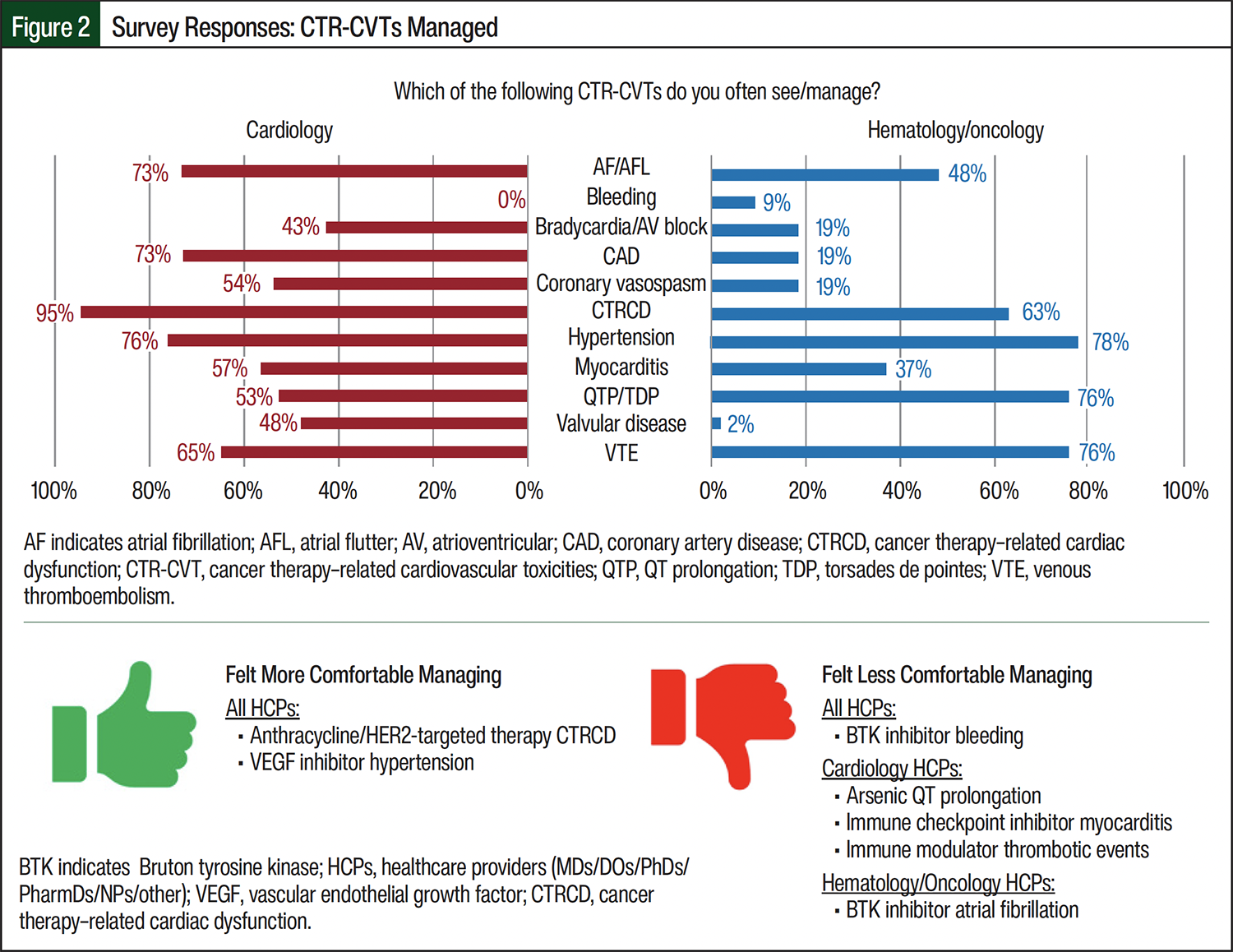
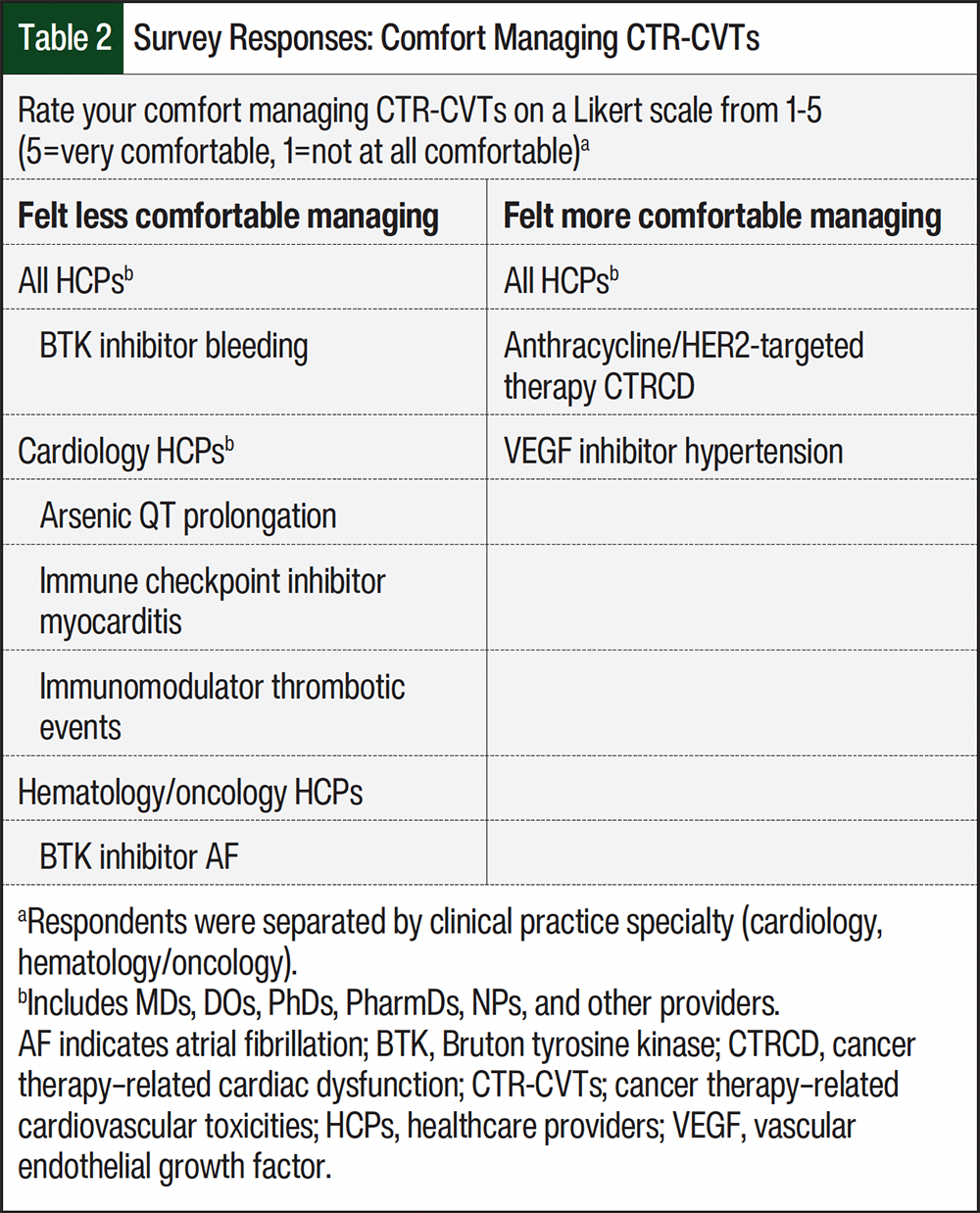
When asked to rate their overall comfort with treating CTR-CVTs on a Likert scale (1-5), with 5 being very comfortable and 1 being not at all comfortable, all HCPs were most comfortable with anthracycline/HER2-targeted therapy–associated CTRCD and VEGF inhibitor–associated hypertension (Table 2). Cardiology HCPs reported being least comfortable treating arsenic-associated QT prolongation, immune checkpoint inhibitor–associated myocarditis, and immune modulator–associated thrombotic events. In contrast, hematology/oncology HCPs reported the least comfort with treating Bruton tyrosine kinase inhibitor–associated AF. For comfort in managing all CTR-CVTs queried, pharmacists reported lower overall scores than nonpharmacists.
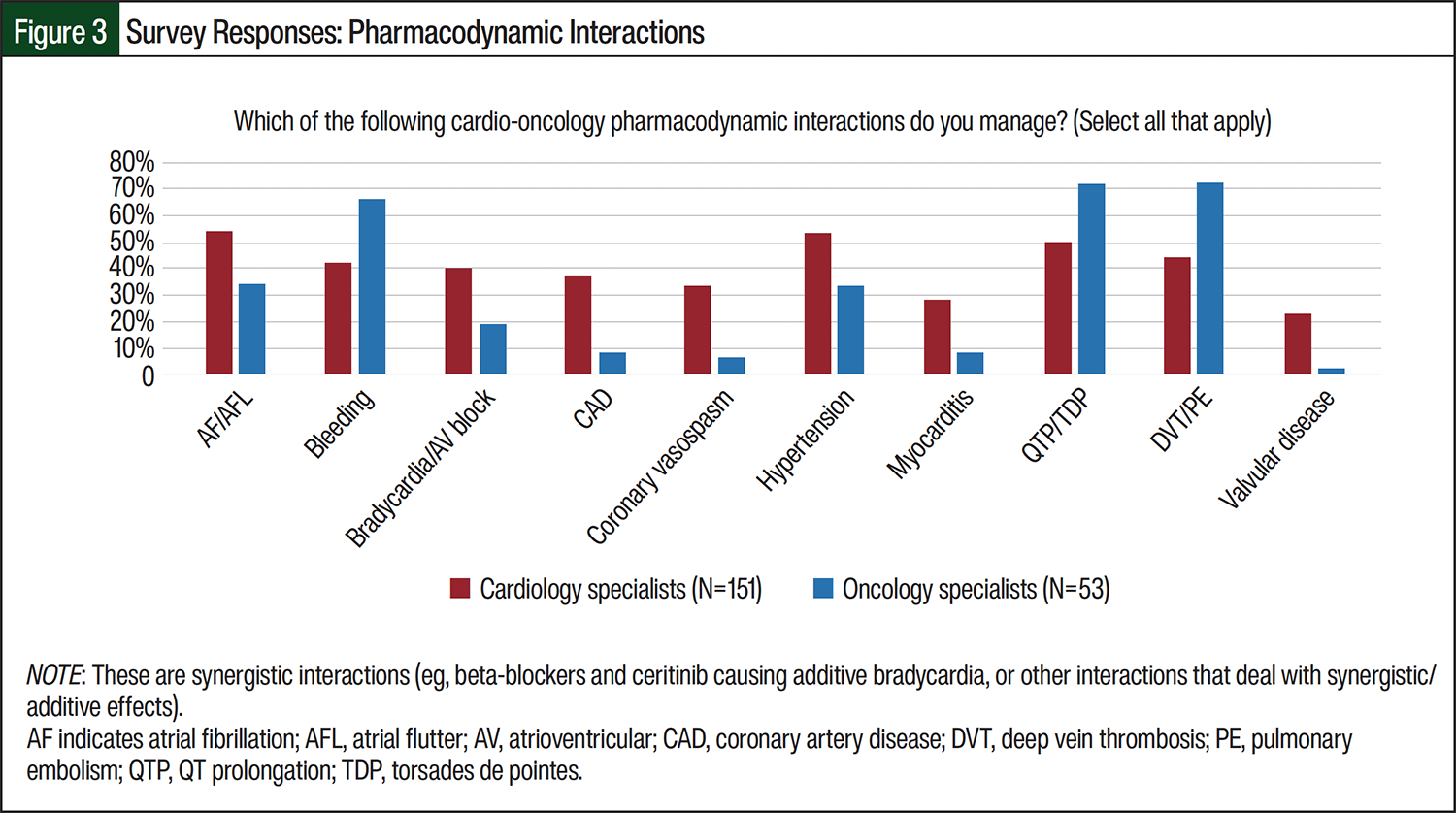
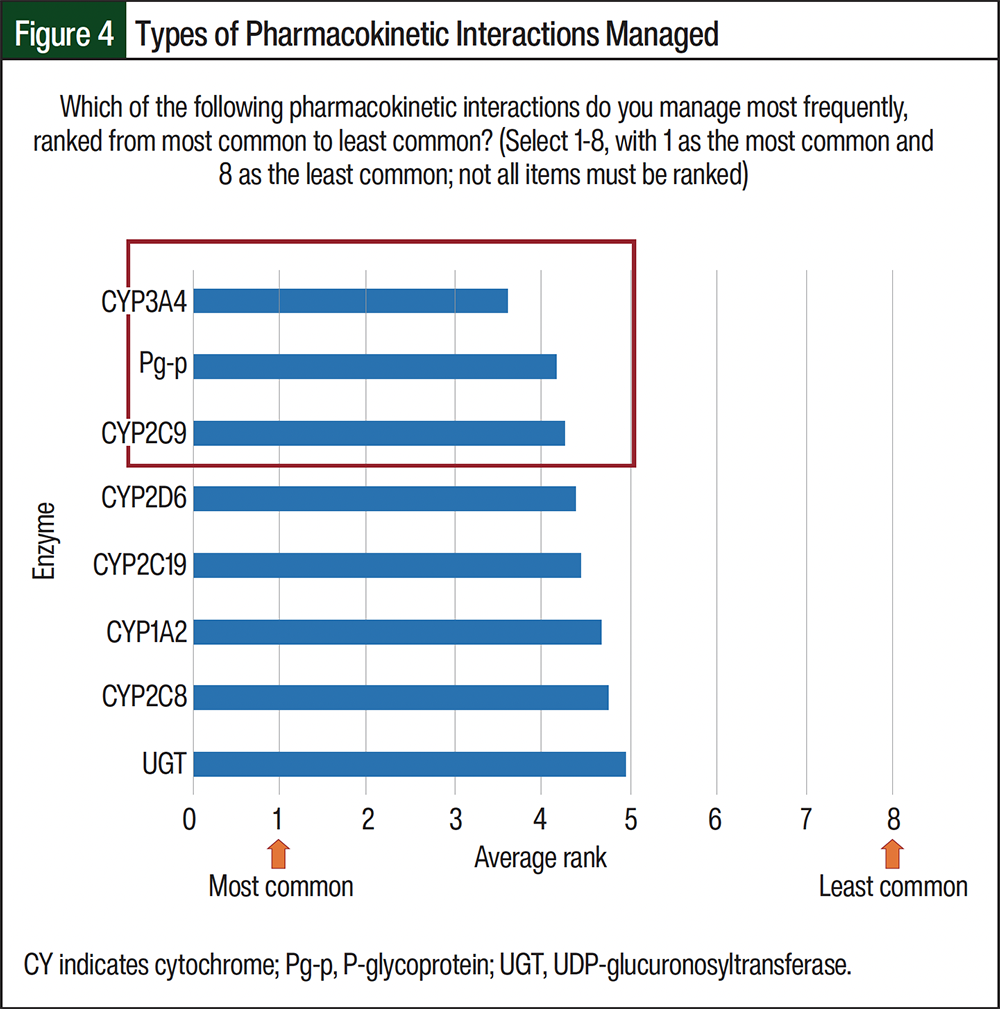
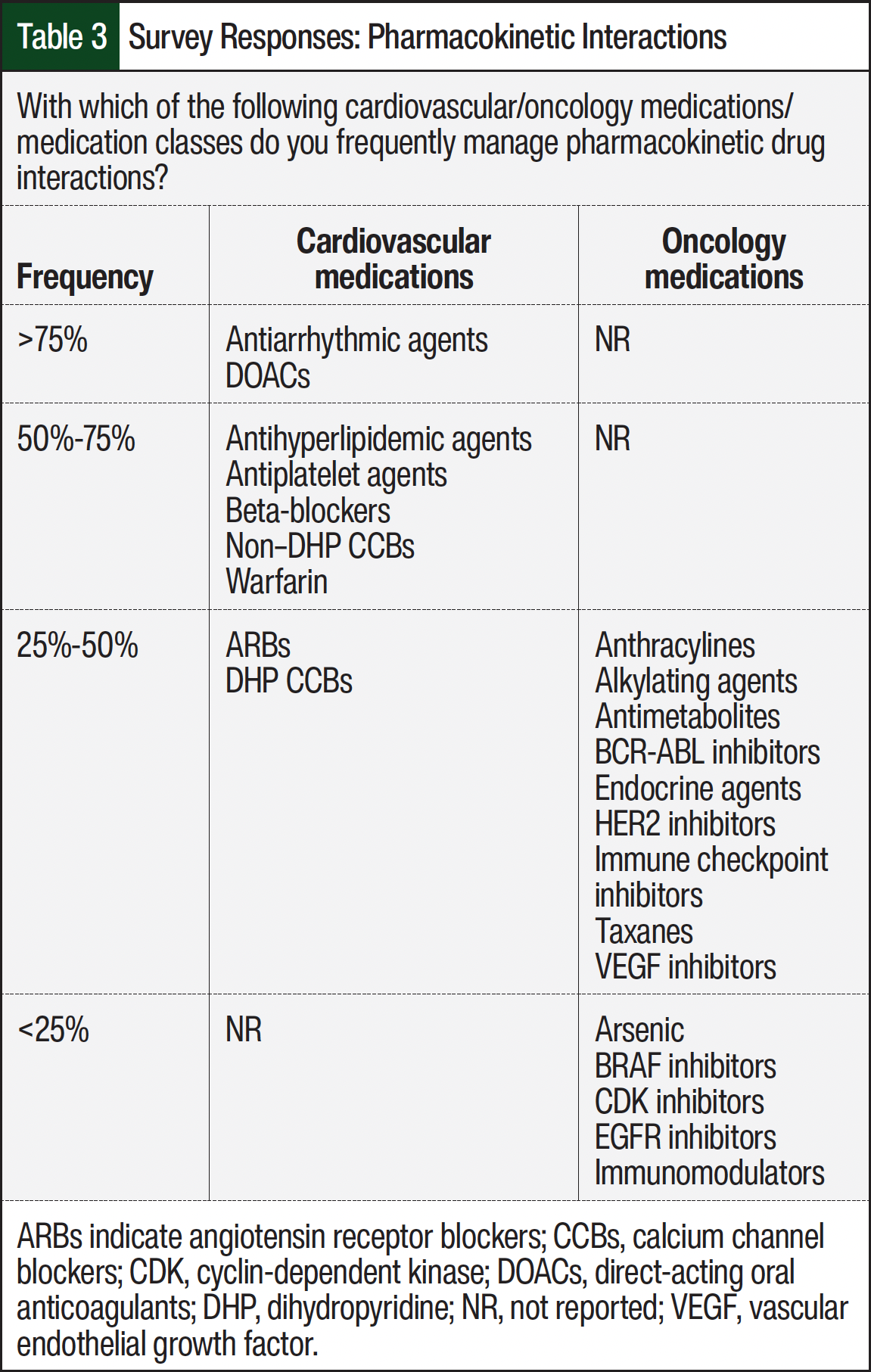
The most common cardio-oncology–related pharmacodynamic (PD) drug–drug interactions (DDIs) encountered were bleeding, hypertension, QT prolongation/torsades de pointes, and deep vein thrombosis/pulmonary embolism, and each of these was more often reported by hematologists/oncologists (Figure 3). The most prevalent types of pharmacokinetic (PK) DDIs were cytochrome (CY)P4503A4 and P-glycoprotein followed by CYP2C9 (Figure 4). Overall, cardiovascular (CV) therapies were more often associated with PK DDIs than with oncology therapies. The specific PK DDIs reported by >75% of survey participants were antiarrhythmic agents and direct-acting oral anticoagulants, followed by warfarin, antiplatelet agents, antihyperlipidemic agents, beta-blockers, and nondihydropyridine calcium channel blockers, which were reported by 50% to 75% of the respondents (Table 3). Common PK DDIs with oncology therapies were widespread across 9 medication categories (Table 3). Overall, the survey participants reported similar PD and PK DDIs among pharmacists and other HCPs.
Immune checkpoint inhibitor–associated myocarditis (74%), immune modulator–associated thrombosis/thrombotic events (64%), Bruton tyrosine kinase inhibitor–associated bleeding (58%), and AF (55%) were ranked the highest educational needs. Overall, the survey responses for educational recommendations were similar between pharmacists and other HCPs.
Discussion
The results of the IC-OS Pharmacy Workgroup survey showed that cardiologists and oncologist/hematologists often manage CTR-CVTs, except for bleeding. As anticipated, cardiologists managed these CTR-CVTs more frequently (43%-95%), whereas the management of CTR-CVTs was less common and more variable with oncologists/hematologists (2%-78%). In addition, there were differences in which these provider types felt comfortable with managing various CTR-CVTs. Although pharmacists and other HCPs felt comfortable managing anthracycline/HER2 agent–associated cardiomyopathy and VEGF inhibitor–associated hypertension, pharmacists felt more comfortable with immune modulator–associated thrombosis/thrombotic events, whereas other HCPs felt more comfortable with ibrutinib/other-associated atrial fibrillation.
There continues to be a steady decline in cancer-related mortality, and treatment-related adverse events (AEs), such as CTR-CVT, negatively impact the long-term morbidity and mortality outcomes of patients with cancer.2 The results of this study support notable differences between cardiology and hematology/oncology HCPs in CTR-CVT management and knowledge gaps. As cardio-oncology continues to develop as a specialty, there is a need to ensure that appropriate educational structures are devised to assure a competent cardio-oncology HCP workforce, including cardiology- and oncology-trained providers, as well as physician extenders, such as pharmacists, nurse practitioners, and physician assistants. With cardio-oncology care strategies ranging across the continuum of care from primary prevention to survivorship and involving a wide range of interdisciplinary teams, guidelines and education should also span across these various healthcare disciplines.
With the exception of a limited cardio-oncology fellowship for cardiologists, there are currently no other structured training programs that provide specific foundational knowledge and training in cardio-oncology. At best, for example, a pharmacist could complete a cardiology residency and take some oncology electives or vice versa.8 Beyond this, there are only traditional education and various medical association meetings to obtain knowledge on these topics. Furthermore, although various practice models for select members of the cardio-oncology team have been published, these are limited in number, and current cardio-oncology program descriptions only briefly describe the roles for ancillary team members, such as pharmacists.9-12 As the scope of practice for pharmacists and other allied health team members continues to rapidly evolve, continuing education may fill a gap while training programs are developed.13-15
In 2020, the Cardio-Oncology Leadership Council of the American College of Cardiology published a perspective regarding training and education in relation to cardio-oncology.16 Although the concept of the document was focused on the physician, the framework is applicable to all HCPs in the cardio-oncology space. The researchers identified that all clinicians, irrespective of training background, must have a core knowledge of CV-related AEs of cancer therapies; the CV risk evaluation before, during, and after cancer treatment; and the unique management aspects of CV disease in patients diagnosed with cancer, such as DDIs. In addition, the researchers proposed a framework that included early education regarding the convergence of the 2 categorical disease states in the respective health degree programs, as well as any postgraduate training programs. This would be further developed into specialty training experiences during general residency and/or fellowship. The education training here would consist of didactic lectures, as well as hands-on experiences. Likewise, this type of training would be foundational for continued education the clinician has transitioned to practice. Last, the proposition of the researchers is to ultimately devise a dedicated specialty training program, albeit residency or fellowship, that provides focus on the cardio-oncology patient population. Beyond training programs, the researchers propose that continual education, delivered through various formats and covering the topics of need, be developed to provide additional or alternative means for cardio-oncology training. This concept of life-long learning could be devised through professional organizations and education providers.16 A similar framework has been devised by Brown and colleagues.17
Given the need for training, as outlined above in the 2 previously mentioned frameworks,16,17 our survey provides evidence for short-term needs via the specific topics, as well as more broadly supports the notion of more structured training for all of the HCPs who manage these patients, including pharmacists. The IC-OS Cardio-Oncology Knowledge Exam could serve as a framework to develop an appropriate training curriculum and program because it is available to physicians, nurses, nurse practitioners, and pharmacists. To qualify for the 60 multiple-choice question examination, applicants must have at least 3 years of education efforts (ie, continued education courses, webinar participation, conference attendance) and 3 years of clinical experience within a multidisciplinary team in which they are engaged in clinical decision-making. In addition, the European Society of Cardiology has recently proposed a framework of a core curriculum to promote the standardization and harmonization of training and evaluation in cardio-oncology.18
After formal training, the need for continuing education cannot be overemphasized given the accelerated pace at which new cancer therapies are arriving on the market. Professional organizations, such as IC-OS, may use the results of internal surveys (eg, postconference evaluations) or external surveys, such as the one presented here, to gain a better understanding of providers’ perceived educational needs. In addition, to ease administration, these surveys can be more routinely administered to capture evolving needs as new cancer therapies and related CVTs emerge. These benefits must be balanced with various limitations, several of which are cited below. Beyond the use of surveys to guide educational content, other limitations of the current continuing education include the lack of an interdisciplinary nature, because programming often focuses on a singular provider type or setting; potential speaker conflicts with pharmaceutical industry; and limited access if virtual access is not offered.
Limitations
This study has several limitations, most of which are inherent to conducting survey-based research. The use of targeted listservs limited the comprehensive inclusion of all HCPs practicing in these areas. Specifically, the included HCP population lacked sufficient nurse practitioner or registered nurse involvement, which limits the generalizability of cardio-oncology educational needs. Similar to the earlier surveys conducted and inherent to the field of cardio-oncology, most of the respondents specialized in cardiology.
Also, the use of “manage” may be interpreted differently by various provider types (eg, pharmacist input requested on steroid dosing for myocarditis), and this may lead to under- or overreporting of the volume of cardiotoxic therapies managed. Provider comfort with managing select aspects of care is not a sole or direct reflection of education gaps or needs, but could result from other factors (eg, inherent seriousness or typical presenting severity of a given CTR-CVT, issues with optimal multidisciplinary management in a given hospital/clinic system).
Finally, the survey did not address the perception of the HCPs on the impact that CTR-CVTs have on oncologic outcomes for patients, which would be a way to measure the perceived impact of value of education and training on outcomes.
Conclusion
Future continuing education efforts should focus on areas in which HCPs feel least comfortable managing CTR-CVTs. Our survey demonstrated that immune checkpoint inhibitor–associated myocarditis, immune modulator–associated thrombosis/thrombotic events, Bruton tyrosine kinase inhibitor–associated bleeding, and AF were ranked the highest regarding educational needs. Furthermore, survey responses for educational recommendations were similar between pharmacists and other HCPs. Because of the constant change within the field of cardio-oncology and the continued rapid development of novel cancer therapies with associated cardiotoxicities, future surveys are necessary to inform constructive educational efforts and direct best clinical practice. In addition, more structured training and consideration of a core curriculum that would allow for standardization of training and evaluation in cardio-oncology for HCPs who manage these patients, including pharmacists, should be considered as this field continues to evolve.
Author Disclosure Statement
Dr Kaspari is an employee at United Therapeutics Corp; Dr Moore is a consultant to AstraZeneca, Lilly, Novartis, Genentech/Roche, and Pfizer; Dr Hayes has served as a speaker for Pharmacy Times and Sanofi Pharmaceuticals; Dr Skersick is an employee at MorphoSys AG and was previously employed at GlaxoSmithKline; Dr Truitt is an employee at and owns stock in United Therapeutics Corp; Dr Beavers, Dr Santiago, Dr Yaseen, Dr Casselli, and Dr Rodgers have no conflicts of interest to report.
References
- Lythgoe MP, Desai A, Gyawali B, et al. Cancer therapy approval timings, review speed, and publication of pivotal registration trials in the US and Europe, 2010-2019. JAMA Netw Open. 2022;5:e2216183.
- Lyon AR, López-Fernández T, Couch LS, et al. 2022 ESC guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 2022;43:4229-4361. Erratum in: Eur Heart J. 2023;44:1621.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): survivorship. Version 2.2025. May 23, 2025. Accessed July 16, 2025. www.nccn.org/professionals/physician_gls/pdf/survivorship.pdf
- Armenian SH, Lacchetti C, Barac A, et al. Prevention and monitoring of cardiac dysfunction in survivors of adult cancers: American Society of Clinical Oncology clinical practice guideline. J Clin Oncol. 2017;35:893-911.
- Curigliano G, Lenihan D, Fradley M, et al. Management of cardiac disease in cancer patients throughout oncological treatment: ESMO consensus recommendations. Ann Oncol. 2020;31:171-190.
- Sulpher J, Mathur S, Lenihan D, et al. An international survey of health care providers involved in the management of cancer patients exposed to cardiotoxic therapy. J Oncol. 2015;2015:391848.
- Peng J, Rushton M, Johnson C, et al. An international survey of healthcare providers’ knowledge of cardiac complications of cancer treatments. Cardiooncology. 2019;5:12.
- Einsfeld L, do Canto Olegário I, Fagundes ML. Intersecting care through specialized pharmacists: a case report of residency rotation focused on the new horizon of cardio-oncology. Curr Pharm Teach Learn. 2023;15:508-513.
- Merali A, Anwar M, Boyd JM, et al. Exploration of current pharmacy practice in cardio-oncology: experiences & perspectives. J Oncol Pharm Pract. 2023;29:1844-1852.
- Yaseen IF, Farhan HA. Cardiovascular drug interventions in the cardio-oncology clinic by a cardiology pharmacist: ICOP-Pharm study. Front Cardiovasc Med. 2022;9:972455.
- Fradley MG, Wilcox N, Frain I, et al. Developing a clinical cardio-oncology program and the building blocks for success: JACC: CardioOncology How To. JACC CardioOncol. 2023;5:707-710.
- Bloom MW, Ferrari AM, Stojanovska J, et al. Cardio-oncology program building: a practical guide. Cardiol Clin. 2025;43:195-207.
- The role of hematology/oncology pharmacists. Hematology/Oncology Pharmacy Association. August 22, 2014. www.hoparx.org/documents/78/HOPA_About_Hem_Onc_Pharmacist_Issue_Brief_FINAL1.pdf
- Scope of hematology/oncology pharmacy practice. Hematology/Oncology Pharmacy Association. 2013. www.hoparx.org/documents/111/HOPA13_ScopeofPracticeBk1.pdf
- Holle LM, Segal EM, Jeffers KD. The expanding role of the oncology pharmacist. Pharmacy (Basel). 2020;8:130.
- Alvarez-Cardona JA, Ray J, Carver J, et al. Cardio-oncology education and training: JACC Council Perspectives. J Am Coll Cardiol. 2020;76:2267-2281.
- Brown SA, Yang EH, Branch M, et al. Training and career development in cardio-oncology translational and implementation science. Heart Fail Clin. 2022;18:503-514.
- López-Fernández T, Farmakis D, Ameri P, et al. European Society of Cardiology core curriculum for cardio-oncology. Eur J Heart Fail. 2024;26:754-771.