Carboplatin has been approved by the US Food and Drug Administration for the treatment of ovarian cancer and has been used off-label for the treatment of many solid tumors, including lung, head and neck, endometrial, breast, and cervical cancers.1 As a nonclassical alkylating agent, carboplatin acts by covalently binding to DNA, thereby interfering with the crosslinking and synthesis of DNA and cell replication. Carboplatin is excreted almost exclusively by the kidneys. Approximately 65% to 70% of the total platinum dose is eliminated as intact carboplatin in the urine during the first 12 to 16 hours after administration.1
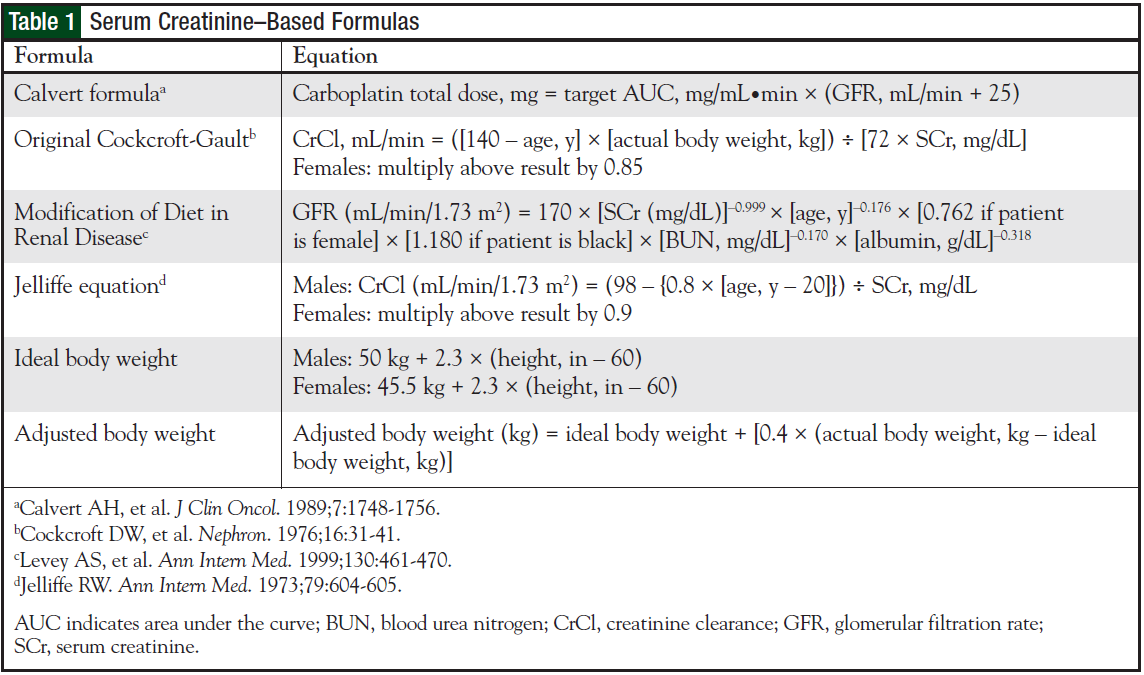
Carboplatin dosage relies on glomerular filtration rate (GFR) and area under the curve (AUC). The Calvert formula is the preferred method to calculate the dose for a given target AUC.2 Serum creatinine (SCr)-based formulas are used to estimate GFR when calculating carboplatin dosage with the Calvert formula. Individualized dosing is the current practice to control plasma drug exposure of carboplatin. A limitation of the Calvert formula is that the carboplatin dosage can substantially vary, depending on the SCr-based formula used to estimate GFR (ie, Cockcroft-Gault, Jelliffe, or Modification of Diet in Renal Disease [MDRD]).
Furthermore, in overweight and obese populations, body weight (actual body weight vs ideal body weight) applied to an SCr-based formula may overestimate GFR. Overestimation of GFR may result in differences in carboplatin dosage that correlate with clinically relevant events, such as dose-limiting thrombocytopenia, treatment delays, and dose reductions. A study by Herrington and colleagues demonstrated that the optimal weight for overweight and obese patients in SCr based formulas for use in the Calvert formula was adjusted body weight.3 The use of actual body weight in overweight or obese patients resulted in a carboplatin AUC that was 30% to 40% higher than the predicted or targeted carboplatin AUC.3
There are scarce data to guide decision-making regarding the influential variables within the Calvert formula (Table 1). Existing literature is currently limited, 4-6 and there is not an established consensus within the oncology community. When actual body weight is applied to an SCr-based formula for use in the Calvert formula, overweight and obese patients may have carboplatin AUCs greater than targeted because of overestimation of renal clearance. The purpose of our study was to evaluate carboplatin dosing in overweight and obese patients and to assess clinical outcomes at our institution.
Study Objectives
The primary objective of this retrospective analysis was to evaluate physician prescribing practices with the Calvert formula in overweight and obese patients within our institution. Specifically, we identified the SCrbased formula used by the physician prescriber to estimate the GFR and body weight (ie, actual, ideal, adjusted) applied to the SCr-based formula, and whether a maximal/capped creatinine clearance (CrCl) rate was determined at the discretion of the prescriber.
This information was gathered from a preprinted chemotherapy order form that included calculations for estimated renal function and the body weight descriptor applied. The secondary objectives were to identify the presence of grade 3 or 4 thrombocytopenia (25.0-49.9 × 10e9/L or <25 × 10e9/L) according to the National Cancer Institute (NCI) Common Toxicity Criteria for Adverse Events,7 dose modifications, and treatment delays caused by toxicity.
Methods
This study was reviewed and approved by the University of Maryland Institutional Review Board. A retrospective analysis was conducted using data from patients who received carboplatin therapy during the period between January 2008 and January 2009. Inclusion criteria were adult patients (aged ≥18 years) who received at least 1 dose of carboplatin with documentation of desired carboplatin AUC for solid tumor malignancies either as monotherapy or as part of com bination chemotherapy treatment. Exclusion criteria included patients with incomplete or missing laboratory parameters on the preprinted chemotherapy order form. Patient data were accessed through electronic medical records. Data collection included demographic information, pretreatment and posttreatment complete blood count and nadir, concurrent cytotoxic chemotherapy, and any supporting documentation confirming treatment delays and dose reductions.
We defined treatment delays as ≥7 days from the planned day of carboplatin administration. A dose reduction was defined as a ≥20% dose decline or a reduction in the target AUC from the previous dose, with supporting documentation on the chemotherapy order confirming a dose reduction secondary to toxicity. The actual carboplatin AUC and actual GFR were not measured as part of this analysis. Stable kidney function was defined by SCr change from baseline of <0.5 mg/dL.8
The SCr-based formula utilized by the prescribing physician, the body weight applied to the formula, the target AUC, and the treatment cycle number were collected from the chemotherapy order. Patients were categorized based on actual body weight (kg) and height (cm) into 1 of 5 groups, including:
- Low body weight: body mass index (BMI) <18.5 kg/m2
- Normal/ideal body weight: BMI 18.5-24.9 kg/m2
- Overweight: BMI 25-29.9 kg/m2
- Obese class I: BMI 30-34.9 kg/m2
- Obese class II: BMI 35-39.9 kg/m2
- Extreme obesity/class III: BMI >40 kg/m2.
Body weight categories are based on the National Institutes of Health guidelines on the identification of overweight and obese adults.9 Study analysis for end points included overweight, obese, and extremely obese patients.
Results
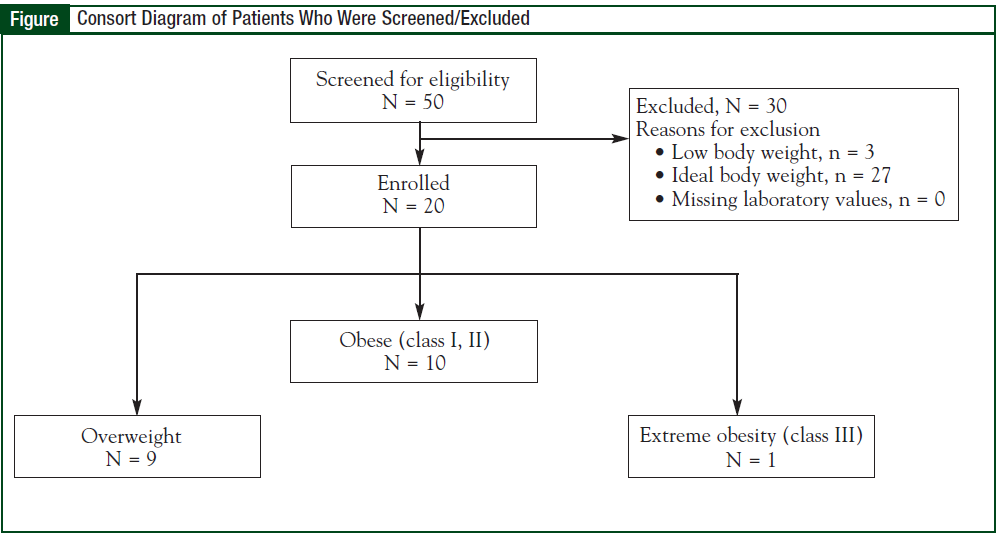
A sample of 50 patients who received carboplatin during the study period were screened for eligibility, and more than 10 medical oncology prescribers dosed carboplatin with the Calvert formula. Thirty patients were excluded based on criteria for low body weight, ideal body weight, or missing laboratory parameters; therefore, 20 patients were included in the final analysis (Figure).
The demographics and baseline laboratory values of the patients are described in Table 2. The study demographics included mean age of 62.3 years, and more whites than blacks comprised the study population.
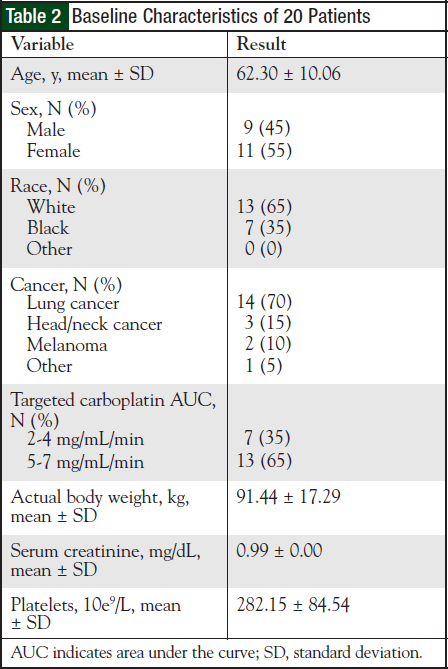
Most patients had a primary diagnosis of non–smallcell lung cancer, followed by malignancy of the head and neck.
Fifty percent of the patients were obese, and the mean BMI was 32.059 kg/m2. Based on the target carboplatin AUC, more than two thirds of patients were prescribed a carboplatin target AUC ≥5 mg/mL/min. Kidney function was stable for all patients.
Seventy percent of the patients (N = 14) were treated with doublet-combination chemotherapy, and the remaining 30% of patients (N = 6) received a triplecombination chemotherapy regimen. The doubletcombination regimens included paclitaxel (N = 8), gemcitabine (N = 3), pemetrexed (N = 2), and etoposide (N = 1). The triple-combination chemotherapy regimens included paclitaxel (N = 5) and gemcitabine (N = 1) to monoclonal antibodies such as bevacizumab, cetuximab, and an investigational agent.
Physician prescribers used the Cockcroft-Gault formula to estimate GFR for use in the Calvert formula in 100% of the patients (N = 20). Prescribers applied the laboratory-derived SCr to all SCr-based formulas. Prescribers did not apply an adjusted SCr value to account for the influence of muscle mass on creatinine concentrations in the elderly.
Actual body weight was applied to the SCr-based formula in 19 patients (95%). Mean body weight was applied to the SCr-based formula in 1 patient. Of note, this patient was extremely obese with a BMI of 48.5 kg/m2.
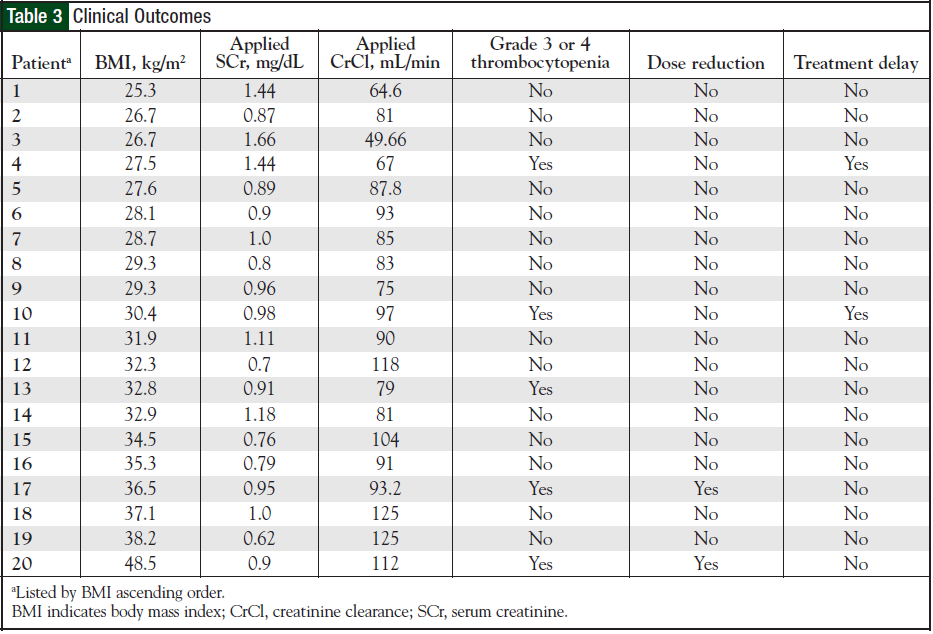
A maximum/capped CrCl rate of 125 mL/min was used for 2 patients (10%). Both of these patients had calcu lated GFR estimates of >150 mL/min based on the Cockcroft- Gault formula, and these patients were enrolled in clinical protocols with amendments for capping CrCl rates. Five patients (25%) experienced grade 3 or 4 thrombocytopenia, 2 patients (10%) experienced a carboplatin treatment delay secondary to toxicity, and these 2 patients subsequently were discontinued from treatment with carboplatin.
In addition, 2 patients (10%) had a documented carboplatin dose reduction secondary to grade 3 or 4 thrombocytopenia. Overall, there were 9 documented clinical events occurring in 5 (25%) of the patients (Table 3).
Discussion
An accurate assessment of kidney function is necessary and vital for determination or modification of dosages of chemotherapy agents eliminated through the kidney in an effort to minimize toxicity and maximize efficacy. Traditionally, CrCl has been measured using 12- or 24-hour urine collections for creatinine or using contrast agents such as iohexol or radiolabeled agents. The clearance of chromium 51-ethylenedi aminetetraacetic acid (51Cr-EDTA) was originally used for the determination of the GFR in the Calvert formula2. This method is costly and may be clinically impractical; therefore, GFR is usually estimated from SCr-based formulas.10-12
Although these formulas are convenient to use, and they conserve time, there is a trade-off in accuracy and consistency with regard to the determination of GFR. The literature is limited in terms of guiding decisionmaking within the oncology community for addressing the influential variables within the Calvert formula in overweight and obese patients.
Our results demonstrate that physician prescribers utilized the Cockcroft-Gault equation to estimate GFR in all patients. None of our prescribers utilized the MDRD or the Jelliffe formula to estimate GFR. The Jelliffe equation is used by most gynecologic oncology group protocols, and gynecologic malignancies did not comprise our study population, which explains why the equation may not have been used.
Existing data comparing the Cockcroft-Gault equation and the MDRD equation for calculating estimated renal function in the Calvert formula were recently published. Shord and colleagues conducted a retrospective analysis to determine the absolute difference between the dose of carboplatin administered using traditional SCr-based formulas to estimate GFR versus the dose calculated based on the MDRD equation.13 Results showed a carboplatin AUC dose divergence in 48% of the patients, yet the frequency of neutropenia, thrombocytopenia, and dose modifications were similar between the 2 groups using either the SCr-based formulas or the MDRD equation to estimate GFR value. The investigators concluded that the traditional SCr-based formulas used to calculate carboplatin dosage should be used until more data become available regarding the use of the MDRD equation in this population.13
The study conclusions are limited, because the goal was not specifically to evaluate dose divergence and clinical outcomes in overweight and obese patients, but the study does provide some data regarding surrogate markers within the Calvert formula.
The NCI’s Cancer Therapy Evaluation Program released 2 action letters in October 2010 to address carboplatin dosing on sponsored protocols and the recent increase in toxicity.14,15 The program recommends utilizing the Cockcroft-Gault equation for calculating CrCl, and commented that the GFR used in the Calvert formula to calculate AUC-based dosing should not exceed 125 mL/min, in an attempt to prevent the erroneous overprediction of renal function estimates when using actual weight in the Cockcroft-Gault equation.
These initiatives are limited, because they do not address the body weight that should be applied to the Cockcroft-Gault equation in special populations of overweight and obese patients. Our prescribers applied actual body weight to the Cockcroft-Gault SCr-based formula in 95% of patients. In our study, applying actual body weight to estimate GFR for use in the Calvert formula did correlate with a high percentage of clinical events, including grade 3 or 4 thrombocytopenia and dose reductions secondary to toxicity.
The study by Herrington and colleagues demonstrated that the optimal weight to use for obese patients, defined as a BMI >30 kg/m2 with renal function and SCr within normal limits, was adjusted body weight.3 Using actual body weight in SCr-based formulas for the Calvert formula resulted in carboplatin AUCs 30% to 40% higher than predicted or targeted AUCs.3 The study results are limited because, despite evaluating actual versus targeted carboplatin AUC divergence in overweight and obese patients, the investigators did not objectively evaluate the impact of a supratherapeutic carboplatin AUC on clinical outcomes, such as doselimiting myelosuppression or treatment delays.3
Ekhart and colleagues assessed the utility of alternative weight descriptors in the Cockcroft-Gault equation to more accurately predict carboplatin clearance in special body weight populations.5 The results demonstrated that adjusted body weight was the best weight descriptor in overweight and obese patients. The study results suggested that overweight and obese patients with normal renal function should receive a flat carboplatin dose based on population carboplatin clearance.
Existing data suggest a strong correlation between carboplatin AUC and dose-limiting myelosuppression, specifically thrombocytopenia.16-18 The incidence of thrombocytopenia in our study population was higher compared with those of standard populations. Based on data from Jodrell and colleagues in patients with ovarian cancer, the expected incidence of grade 3 thrombocytopenia for carboplatin AUC 4 to 5 is 5%, AUC 5 to 6 is 10%, and AUC 6 to 7 is 20%.19
Limitations
There are some limitations to our investigation. This was a retrospective study design, and we were not able to control for the heterogeneity that comprised our small study population.There was also inconsistency with regard to the number of carboplatin treatment cycles that patients received in relation to documented dose reductions or treatment delays.
Inconsistency also occurred with the time at which the complete blood count and nadir(s) were taken and evaluated for each patient. The chemotherapy combination regimens that each patient received were not well balanced, thus the addition of other cytotoxic chemotherapy agents, such as paclitaxel, increases the risk and severity of myelosuppression when compared with monotherapy. We did not identify any independent risk factors predicting dose reductions or therapy delays resulting from toxicity (ie, race, sex, age, cancer diagnosis, baseline platelet count, and previous myelotoxic chemotherapy, concurrent radiation therapy, or performance status).
Finally, we did not measure actual carboplatin AUC or actual GFR utilizing 51Cr-EDTA.
Conclusion
Despite the study limitations, our results contribute to existing data regarding prescribing patterns within our institution and highlight unique considerations when calculating carboplatin dosage with the Calvert formula in overweight and obese patients. The use of actual body weight to estimate GFR in relation to the Calvert formula was associated with a high percentage of adverse clinical events.
Increased awareness and education regarding unique considerations with the Calvert formula in overweight and obese populations should be directed to medical oncology physician prescribers, pharmacists, and healthcare providers within the oncology community to establish quality assurance within the institution or practice site. Future considerations include designing a prospective study evaluating body weight descriptors (ideal vs adjusted) to estimate GFR for use in the Calvert formula incorporating measured carboplatin AUCs compared with target AUCs to identify dose divergence and subsequent adverse clinical events in this population. A prospective study may substantiate these preliminary, clinically relevant data and may be able to establish a consensus in clinical practice, which is critical for patient safety and clinical outcomes.
Author Disclosure Statement
Drs Nightingale, Trovato, Lee, and Thompson have reported no actual or potential conflicts of interest.
References
- Alberts DS, Dorr RT. New perspectives on an old friend: optimizing carboplatin for the treatment of solid tumors. Oncologist. 1998;3:15-34.
- Calvert AH, Newell DR, Gumbrell LA, et al. Carboplatin dosage: prospective evaluation of a simple formula based on renal function. J Clin Oncol. 1989;7:1748- 1756.
- Herrington JD, Tran HT, Riggs MW. Prospective evaluation of carboplatin AUC dosing in patients with a BMI ≥27 or cachexia. Cancer Chemother Pharmacol. 2005;57:241-247.
- Chatelut E, Canal P, Brunner V, et al. Prediction of carboplatin clearance from standard morphological and biological patient characteristics. J Natl Cancer Inst. 1995;19:573-580.
- Ekhart C, Rodenhuis S, Schellens JH, et al. Carboplatin dosing in overweight and obese patients with normal renal function, does weight matter? Cancer Chemother Pharmacol. 2009;64:115-122.
- Schmitt A, Gladieff L, Lansiaux A, et al. A universal formula based on cystatin C to perform individual dosing of carboplatin in normal weight, underweight, and obese patients. Clin Cancer Res. 2009;15:3633-3639.
- Cancer Therapy Evaluation Program. Common Terminology Criteria for Adverse Events, v3.0S. http://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/ctcaev3.pdf. August 9, 2006. Accessed August 19, 2011.
- Thadhani R, Pascual M, Bonventre JV. Acute renal failure (letter). N Engl J Med. 1996;334:1448-1460.
- National Institutes of Health National Heart, Lung, and Blood Institute. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: the Evidence Report. NIH Publication No 98- 4083. September 1998. www.nhlbi.nih.gov/guidelines/obesity/ob_gdlns.pdf. Accessed August 19, 2011.
- Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16:31-41.
- Levey AS, Bosch JP, Lewis JB, et al. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Intern Med. 1999;130:461-470.
- Jelliffe RW. Creatinine clearance: bedside estimate (letter). Ann Intern Med. 1973;79:604-605.
- Shord SS, Bressler LR, Radhakrishnan L, et al. Evaluation of the Modified Diet in Renal Disease Equation for calculation of carboplatin dose. Ann Pharmacother. 2009;43:235-241.
- National Institutes of Health, National Cancer Institute. Action letter for protocols sponsored by the National Cancer Institute that use carboplatin. Letter. October 1, 2010. www.cancerletter.com/downloads/20101008/download. Accessed August 19, 2011.
- National Institutes of Health, National Cancer Institute. Follow-up for information letter regarding AUC-based dosing of carboplatin. Letter. October 22, 2010. http://ctep.cancer.gov/content/docs/Carboplatin_Information_Letter.pdf. Accessed August 19, 2011.
- Duffull SB, Robinson BA. Clinical pharmacokinetics and dose optimization of carboplatin. Clin Pharmacokinet. 1997;33:161-183.
- Sørensen BT, Strömgren A, Jakobsen P, Jakobsen A. Dose-toxicity relationship of carboplatin in combination with cyclophosphamide in ovarian cancer patients. Cancer Chemother Pharmacol. 1991;28:397-401.
- Jakobsen A, Bertelsen K, Andersen JE, et al. Dose-effect study of carboplatin in ovarian cancer: a Danish Ovarian Group study. J Clin Oncol. 1997;15:193-198.
- Jodrell DI, Egorin MJ, Canetta RM, et al. Relationships between carboplatin exposure and tumor response and toxicity in patients with ovarian cancer. J Clin Oncol. 1992;10:520-528.
Dr Nightingale is Assistant Professor, Department of Pharmacy Practice, Jefferson School of Pharmacy, Thomas Jefferson University, Philadelphia, PA; Dr Trovato is Associate Professor, Department of Pharmacy Practice and Science, University of Maryland School of Pharmacy, Baltimore; Dr Lee is Investigational Drug Specialist, Supervisor, Investigational Drug Service Pharmacy, Department of Pharmacy, University of Maryland Medical Center, Baltimore; and Dr Thompson is Investigational Drug Specialist, Investigational Drug Service Pharmacy, Department of Pharmacy, University of Maryland Medical Center, Baltimore. This study was presented as a poster at the 5th Annual Meeting of the Hematology Oncology Pharmacy Association; June 2009; Miami, FL