Connecting Science to Practice
This pilot study explores the use of a wearable continuous
temperature monitoring (CTM) device to detect febrile neutropenia
(FN) in patients with acute myeloid leukemia who
received high-dose cytarabine. By comparing outcomes between
patients using a CTM patch and an historical cohort
using thermometers, the study assessed feasibility, user experience,
and outcomes. Results showed reduced intensive care
unit transfers and fewer infections in the CTM group, although
some patients had technical challenges with the device.
These findings support the feasibility of CTM in outpatient
oncology care and show that further study for its
potential to improve early FN recognition and clinical outcomes
is warranted. This research advances hematology/oncology
pharmacy practice by highlighting the role of digital
health tools, such as CTM devices.
Febrile neutropenia (FN) is a common and potentially life-threatening complication of anticancer therapies. FN is associated with significant preventable complications, including hypotension, acute renal failure, and respiratory or heart failure, occurring in approximately 25% to 30% of patients, and early mortality occurs in as many as 11% of patients.1 Fever may occur well before any clinical signs or symptoms of infection are present.1 Early recognition and prompt intervention of FN is essential because a delay in time to first antibiotic administration is associated with increased mortality.2-5 In the ambulatory care setting, the standard approach is intermittent temperature monitoring (every 4-6 hours). Intermittent temperature monitoring relies on patient self-assessment, which requires strict compliance with the use of an accurate home thermometer. Ambulatory care patients must independently determine when to contact healthcare providers or initiate further care.
The utility of adding biometric data in the ambulatory care setting using noninvasive and continuous monitoring is of interest.6-8 The potential benefits of at-home wearable devices are to detect fever earlier, prompting patients to seek medical care immediately before onset of symptoms and to minimize negative sequela via early identification and treatment.
Continuous temperature monitoring (CTM) via transdermal patch has been reported to detect FN earlier than intermittent manual monitoring in hospitalized patients.9 Conversely, adequate evaluation in the outpatient or ambulatory oncology setting is lacking. A previous feasibility study suggested assessing high-risk populations, including patients undergoing consolidation with high-dose cytarabine (HiDAC) chemotherapy for acute myeloid leukemia (AML) who have achieved remission with intensive induction chemotherapy.10 HiDAC is associated with a significant rate of FN, occurring in ≤70% of patients, and patients are typically provided antimicrobial prophylaxis with granulocyte colony-stimulating factor support while being monitored in the ambulatory care setting after completion of chemotherapy until resolution of neutropenia or adverse events necessitating hospitalization.11,12 Our study examines the feasibility and clinical utility of a remote CTM device in the ambulatory care setting for adult patients with AML who have received intensive consolidation chemotherapy.
Methods
This study was performed in accordance with the principles of the Declaration of Helsinki, and approval was granted by the local institutional review board at Augusta University, Augusta, GA. This was a single-center, prospective study (August 2021 to June 2023) with a retrospective preintervention cohort (September 2019 to July 2021). The patient cohorts included sequential patients aged ≥18 years with a diagnosis of AML who received consolidative HiDAC monotherapy. Anticipated enrollment for the prospective pilot was 20 cycles, targeting approximately 10 patients for approximately 2 cycles each. Anticipated screening for the retrospective cohort was 40 cycles. Patients were excluded if they received additional chemotherapy (eg, oral chemotherapeutic agents such as midostaurin, gemtuzumab ozogamicin) in combination with HiDAC, had FN before discharge, or remained hospitalized for longer than 10 days after HiDAC initiation.
All patients were counseled to check their temperature with an oral thermometer every 4 to 6 hours per usual care. Patients in the prospective cohort signed written informed consent and were provided with CTM devices (TempTraq patches; BlueSparks Technologies Inc), which are noninvasive, disposable, flexible, silicone gel–based adhesive patches. The patches transmit data via Bluetooth connection to smartphone apps, and data are stored on a HIPAA-secure web-based platform. Each patch provides CTM for 72 hours. Patients were educated on proper patch application (eg, axillary placement) and provided training on the affiliated smartphone app. A smartphone was provided to patients without a compatible device. The first CTM device was placed by the patient on the date of discharge. Patients were instructed to wear the device at all times except for bathing until they achieved neutrophil recovery (1500 cells/µL; maximum 15 days) or until a hospital admission, whichever occurred first. Patients were educated to respond to app alerts promptly, including going to the nearest emergency department for any temperature reading ≥38.3°C or ≥38°C that was sustained for >1 hour. Study investigators, which included pharmacists, advanced practice providers, and a physician, simultaneously monitored the patients’ data in real time 24 hours a day 7 days a week via the clinicians’ smartphone apps using deidentified codes. Clinicians contacted patients for alerts to ensure appropriate actions were taken. Patients were provided with the monitoring clinician’s cell phone number for any troubleshooting. Patients completed an end-of-study questionnaire during their next clinic visit after completion of HiDAC monitoring.
With respect to the chemotherapy regimen, all patients received HiDAC dosed between 1 and 3 g/m2 administered every 12 hours either on days 1, 3, and 5 or on days 1, 2, and 3 at physician discretion. Standard supportive-care measures were provided, including prophylaxis for nausea and vomiting, corticosteroid eye drops, pre-HiDAC dose assessment of neurologic functioning by nursing staff, and discharge prescriptions for infection prophylaxis (eg, ciprofloxacin) and myeloid growth factor support.
Demographic data were collected, and efficacy end points included incidence of fever, emergency department visit and/or hospital admission, sepsis, microbiologically or clinically defined infection, intensive care unit (ICU) admission, hospital and ICU length of stay, and death. Mortality data were reviewed for the 15-day follow-up period after each HiDAC cycle. For patients admitted during that 15-day follow-up period, mortality was also monitored through the end of that hospitalization. Descriptive statistics were used to characterize the population and outcomes of this pilot study.
Results
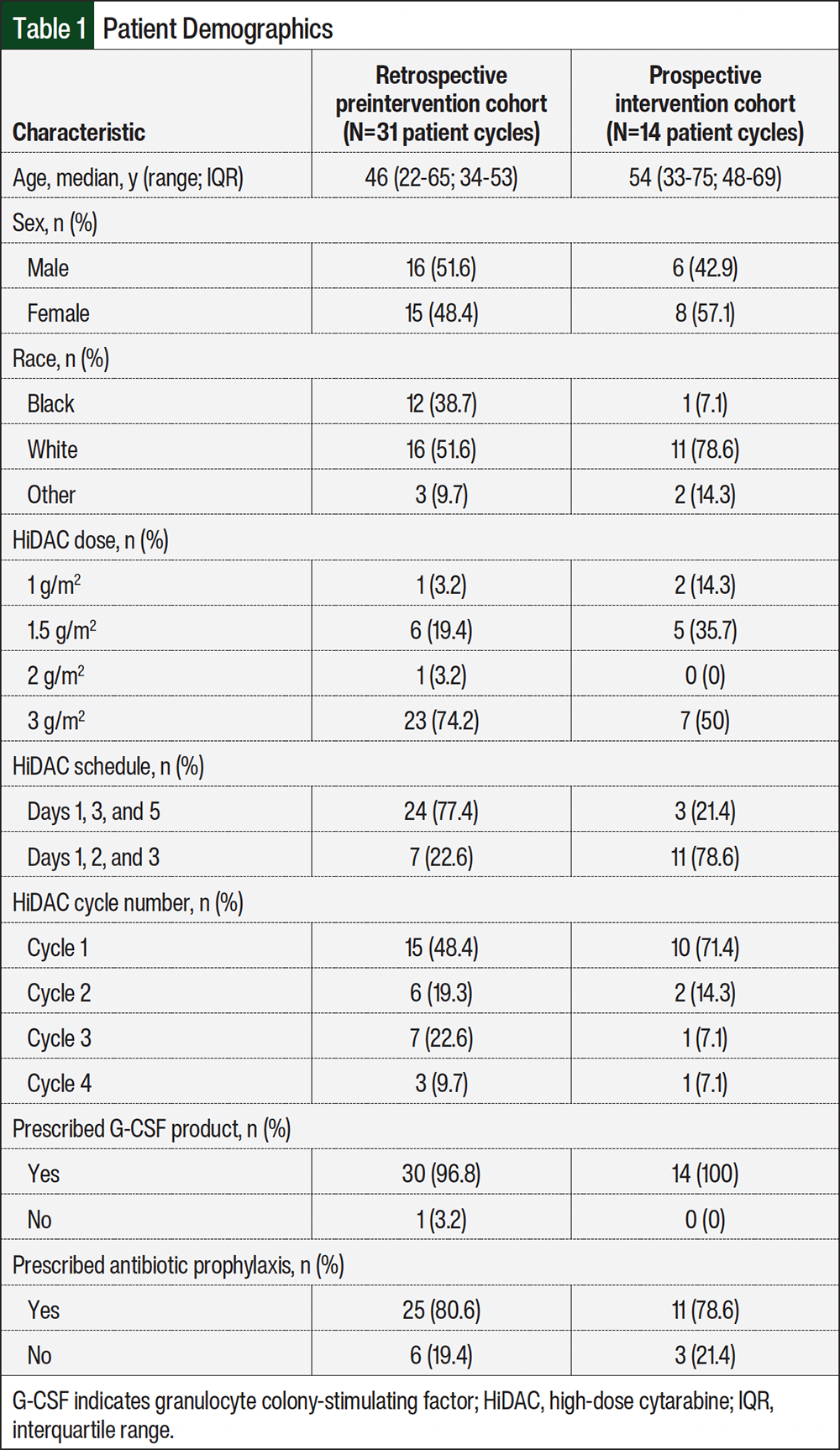
In the retrospective preintervention cohort, a total of 44 cycles were screened, resulting in 31 cycles for 18 patients included in the final analysis. Reasons for exclusion included additional chemotherapy in 10 cycles, not discharged within 10 days in 2 cycles, and diagnosis of chronic myeloid leukemia in blast crisis in 1 cycle.
In the prospective cohort, 17 patients were screened over a total of 22 HiDAC cycles, resulting in 12 patients enrolled over the course of 14 cycles. One patient participating in the study had CTM during 3 cycles of HiDAC. Reasons for screen failure included patient declining enrollment in 6 cycles and ineligibility due to concomitant chemotherapy in 2 cycles.
Demographic data differed between the 2 groups (Table 1). Patients in the prospective cohort were older and more likely to be White, receive HiDAC dose <3 g/m2, to be receiving their first cycle, and to be treated with HiDAC scheduled on days 1, 2, and 3.
In the retrospective cohort, 11 (35.5%) patients had documentation of an admission for FN, but 1 had documentation of admission to an outside facility without detailed records. Incidence of fever without emergency department visit or hospitalization is not reportable in this cohort due to its retrospective nature. Of the 10 evaluable patients, 9 had ≥1 documented infection: Escherichia coli bacteremia (2 patients), Streptococcus viridans bacteremia (2 patients), methicillin-resistant Staphylococcus aureus (MRSA) bacteremia (2 patients), MRSA bacteremia with concomitant Clostridioides difficile (1 patient), COVID-19 (1 patient), and 1 patient with physician documentation of a skin and soft tissue infection that was not microbiologically defined. Of the 10 evaluable patients, 9 met systemic inflammatory response syndrome criteria, 4 of the 10 were transferred to the ICU, and none died (Table 2).
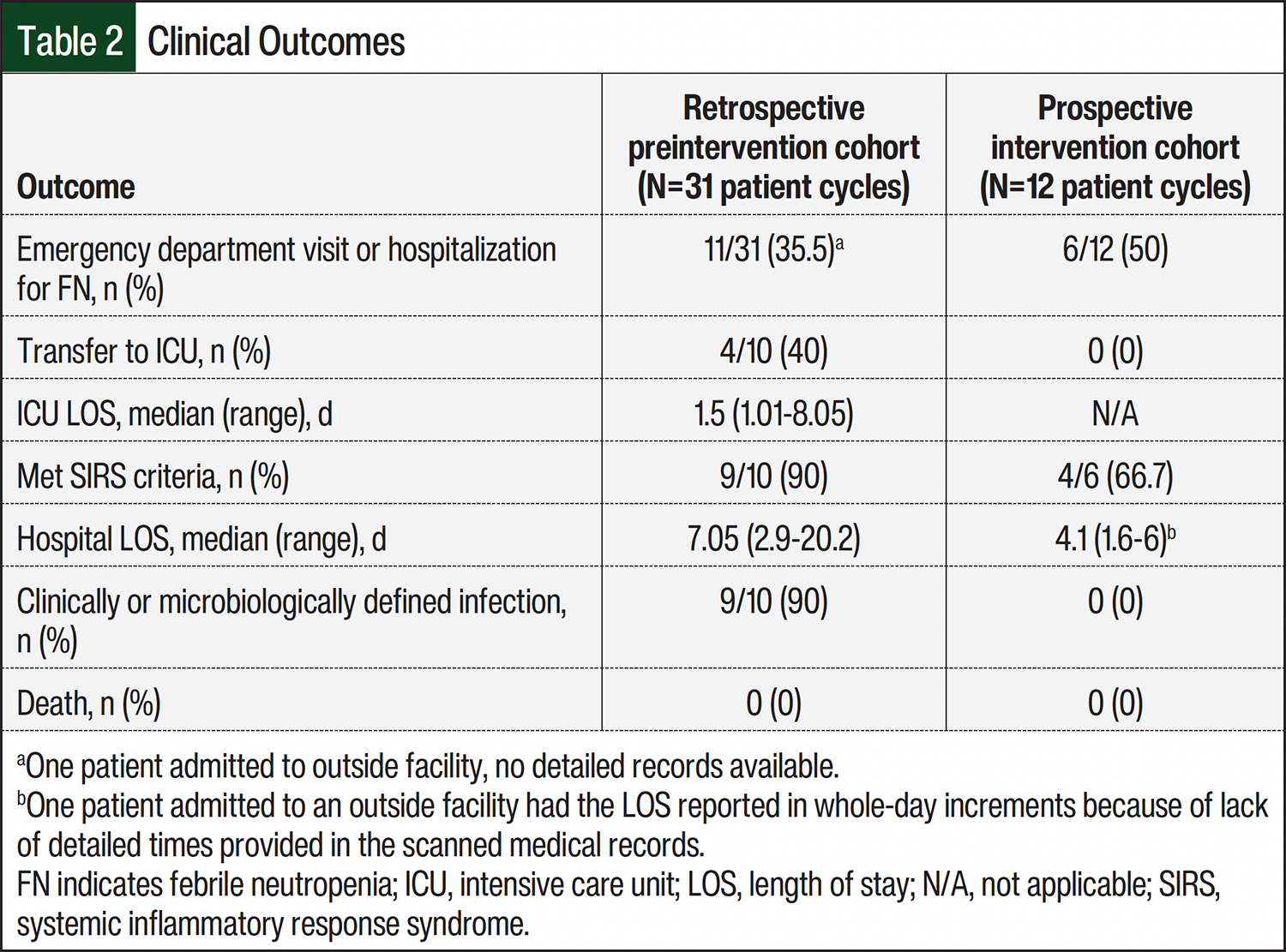
In the prospective cohort, 2 patients withdrew during the study and 1 patient had a ‘no data transmission’ alert and subsequently did not respond to provider attempts to make contact. In the patient with the ‘no data transmission’ alert, the app reported fever immediately after the CTM patch was placed; this was not validated by hospital thermometers, resulting in patient request to withdraw. This resulted in 12 of 14 patient cycles with data reported herein. Of the 12 patient cycles with full data, 4 did not have a fever and 8 had ≥1 fever. Notably, the 1 patient who was enrolled for 3 cycles of HiDAC did have FN after their second and third cycles, and thus accounts for 2 of these episodes reported herein. The incidence of hospitalization for FN was 50% (6 of 12 evaluable cycles) because 2 patients with fever did not follow through on clinician advice to go to the hospital, 1 of whom had documented neutrophil count recovery the following day in clinic. Of the 6 patient cycles with admission for FN, 1 patient went to an outside hospital whereby the discharge summary indicated FN with sepsis. Of the 5 other patient admissions to our facility, none had provider documentation of sepsis, but 3 did meet systemic inflammatory response syndrome criteria with tachycardia and neutropenia. None of the 6 admitted patients were transferred to the ICU, had a microbiologically or clinically defined infection, or died (Table 2).
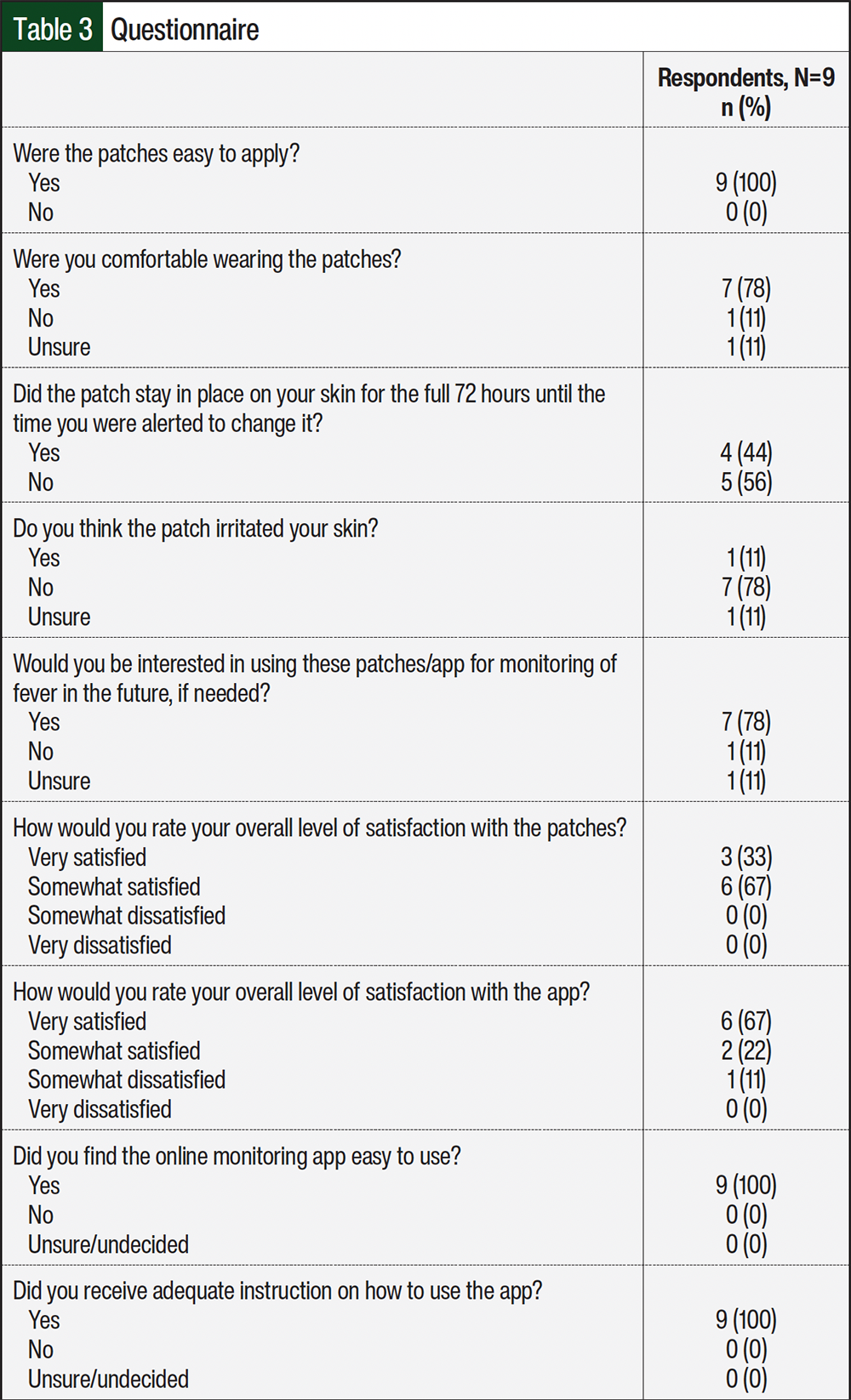
Regarding feasibility in the prospective cohort, only 4 of the 12 patient cycles did not experience any technological issues, whereas the remaining 8 patient cycles had the following: 7 had ≥1 ‘no data transmission’ alert because of various user errors (eg, smartphone not within range, Bluetooth setting turned off), 2 had patch position issues requiring provider assistance, 1 had a malfunction presumed to be due to excessive sweat, and 1 had a patch malfunction consisting of no connection to a device immediately on activation, necessitating new patch placement. Within the prospective cohort, 8 patients completed the questionnaire after 9 cycles. For the remaining 5 patient cycles, the participant either declined to complete the survey or did not return phone calls or return to our facility as they were subsequently managed at a local oncology office (Table 3). Most patients were somewhat satisfied to very satisfied with the device and application overall and were interested in pursuing further monitoring with the CTM process.
Discussion
Despite the use of antimicrobial prophylaxis and myeloid growth factor support, FN remains a significant complication after consolidative chemotherapy for the management of AML. Previous studies evaluating the same CTM device used in our study reported earlier detection of fever compared with the standard of care consisting of intermittent monitoring; however, real-time use of the data was lacking.9,13 In addition, previous exploratory studies using CTM in patients with hematologic malignancies lacked assessment of clinical outcomes.10,14,15 Other feasibility studies also did not use the data in real time or permitted a few hours for providers to respond to alerts during working hours with patients to self-triage after-hours16,17 but recommended wearable devices have data automatically analyzed and available for clinical use,14,18 which was done in our study. Overall, a recent scoping review on wearable devices determined that few (<10%) of the available studies were randomized, controlled trial designs, and most (approximately 43%) focused on user feasibility with very few including assessment of clinical efficacy, highlighting the necessity of further studies in this area, particularly those that include clinical outcomes.6
In this pilot study, the use of a CTM device was associated with a higher incidence of admission for FN than historical rates at our institution. In addition, compared with historical patients, those who used the CTM patch were less likely to be transferred to the ICU, have a confirmed infectious source, and/or had shorter length of hospitalization. Notably, the incidence of FN admission after HiDAC in previous reports ranges from approximately 14% to 70%, similar to our results.11,12,19-21 Larger studies are necessary to evaluate if the use of a CTM device alters this outcome. These data suggest that early detection of fever may mitigate negative clinical outcomes. Future studies should evaluate time to antibiotic initiation to determine impact on outcomes such as sepsis and ICU transfer.
Our study incurred several logistical challenges, including the COVID-19 pandemic disrupting study start-up and enrollment, lower HiDAC utilization in the prospective period potentially based on more timely initiation of allogeneic stem cell transplantation, barriers in enrolling and following up patients from rural areas, and issues with patient ability to follow through on instructions provided in the prospective cohort. Specifically, investigators had to initiate contact with patients numerous times for various issues related to patch placement or replacement and troubleshooting connectivity issues with the patch and smartphone. Previous studies have reported issues with compliance with use of biometric monitoring devices, patient concerns with unnecessary alerts, and concerns related to device placement, including lack of accurate data from improper use of the device.22-24 Because these devices require active and ongoing participation by patients/caregivers, consideration should be given to the disparities that exist with respect to technology literacy and access to broadband, Wi-Fi, and cellular data. Both may prevent inclusivity in further studies or successful implementation in clinical practice for all patients. Technological problems can be demotivating for patient compliance with devices. Future studies of CTM devices or other technology in the ambulatory care setting should carefully consider ease of use and feasibility. Participants who are of older age, lack knowledge of smartphone or app use, lack a compatible smartphone device for the app to run continuously in the background (eg, required a non-iPhone brand), or have low literacy may not benefit from these technological measures without substantial education and ongoing remote supervision by clinicians or support staff. Future studies should investigate how to optimize patient education and provide adequate ongoing support to reduce missing data to enable the best use of this technology. Further, cost of the device and cellular data are real-world barriers patients may encounter with these technologies.
Study Limitations
Limitations of this study include the partial retrospective design, limited number of subjects enrolled, and imbalances in demographic factors. Although no data exist comparing incidence of FN by specific HiDAC dose, the lower percentage of patients with HiDAC dose <3 g/m2 in the prospective cohort could have impacted outcomes.
Conclusion
Limited data from this study suggests that a CTM device in the outpatient setting is potentially feasible. This study preliminarily indicates that the CTM device has certain potential in outpatient monitoring of FN, but further large-scale and high-quality studies are needed for verification. Various technological issues should be considered when implementing this type of device in larger studies. Future studies in inpatient and outpatient settings should focus on determining if CTM devices are correlated with better clinical outcomes and decreased rates of complications related to intensive chemotherapy regimens.
Acknowledgments
All authors contributed to the study conception and design. Material preparation and data analysis were performed by Amber Clemmons and E. Behren Ketchum. Data collection was performed by Amber Clemmons, E. Behren Ketchum, Stephanie Daniels, and Sarah Jimenez. The first draft of the manuscript was written by Amber Clemmons and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding Sources
This work was supported by funding from a Clinical and Translational Research Unit seed grant with additional financial support from the Unite the Fight Against Cancer intramural funding from the Georgia Cancer Center.
Author Disclosure Statement
Dr Jimenez is on the Advisory Board of and has received honoraria from Bristol Myers Squibb, is a consultant at acCELLapy, and has received honoraria from JADPRO; Dr Mian is an Adjunct Assistant Professor in Hematology and Oncology Services at Augusta University; Dr Clemmons has received honoraria from HOPA, PTCE, and the Annenberg Center for Health Sciences; Dr Ketchum, Ms Daniels, and Dr Bryan have no conflicts of interest to report.
References
- Taplitz RA, Kennedy EB, Flowers CR. Outpatient management of fever and neutropenia in adults treated for malignancy: American Society of Clinical Oncology and Infectious Diseases Society of America clinical practice guideline update summary. J Oncol Pract. 2018;14:250-255. doi:10.1200/JOP.18.00016
- Rosa RG, Goldani LZ. Cohort study of the impact of time to antibiotic administration on mortality in patients with febrile neutropenia. Antimicrob Agents Chemother. 2014;58:3799-3803. doi:10.1128/AAC.02561-14
- Koenig C, Schneider C, Morgan JE, et al. Association of time to antibiotics and clinical outcomes in patients with fever and neutropenia during chemotherapy for cancer: a systematic review. Support Care Cancer. 2020;28:1369-1383. doi:10.1007/s00520-019-04961-4
- Salstrom JL, Coughlin RL, Pool K, et al. Pediatric patients who receive antibiotics for fever and neutropenia in less than 60 min have decreased intensive care needs. Pediatr Blood Cancer. 2015;62:807-815. doi:10.1002/pbc.25435
- Fletcher M, Hodgkiss H, Zhang S, et al. Prompt administration of antibiotics is associated with improved outcomes in febrile neutropenia in children with cancer. Pediatr Blood Cancer. 2013;60:1299-1306. doi:10.1002/pbc.24485
- Cloß K, Verket M, Müller-Wieland D, et al. Application of wearables for remote monitoring of oncology patients: a scoping review. Digit Health. 2024;10:20552076241233998. doi:10.1177/20552076241233998
- Majhail NS, Cox T, Larson S, et al. Outpatient administration of chimeric antigen receptor T-cell therapy using remote patient monitoring. JCO Oncol Pract. 2025;21:1601-1608. doi:10.1200/OP-25-00062
- Cox T, Zahradka N, Martin C, et al. Remote patient monitoring for 15 vs. 30 days in outpatient chimeric antigen receptor T-cell therapy (CAR-T) across a large health system. Transplant Cell Ther. 2025;31:S223-S224. Abstract 302. doi:10.1016/j.jtct.2025.01.342
- Flora C, Tyler J, Mayer C, et al. High-frequency temperature monitoring for early detection of febrile adverse events in patients with cancer. Cancer Cell. 2021;39:1167-1168. doi:10.1016/j.ccell.2021.07.019
- Kroloff M, Ramezani R, Wilhalme H, Naeim A. Remote monitoring of patients with hematologic malignancies at high risk of febrile neutropenia: exploratory study. JMIR Form Res. 2022;6:e33265. doi:10.2196/33265
- Elemam O, Zaidi SZ, Al-Humaidi A, et al. Safety of early discharge after high-dose ara C consolidation. J Appl Hematol. 2012;3:67-70.
- Saini L, Minden MD, Schuh AC, et al. Feasibility of outpatient consolidation chemotherapy in older versus younger patients with acute myeloid leukemia. Am J Hematol. 2012;87:323-326. doi:10.1002/ajh.22268
- Nessle CN, Flora C, Sandford E, et al. High-frequency temperature monitoring at home using a wearable device: a case series of early fever detection and antibiotic administration for febrile neutropenia with bacteremia. Pediatr Blood Cancer. 2022;69:e29835. doi:10.1002/pbc.29835
- Jacobsen M, Rottmann P, Dembek TA, et al. Feasibility of wearable-based remote monitoring in patients during intensive treatment for aggressive hematologic malignancies. JCO Clin Cancer Inform. 2022;6:e2100126. doi:10.1200/CCI.21.00126
- Khan SN, Tewari M, Lee S, et al. High-frequency temperature monitoring detects clinically actionable fevers otherwise missed by standard-of-care monitoring during treatment of hematologic malignancies. Blood. 2024;144(suppl 1):7500. doi:10.1182/blood-2024-194678
- Verma N, Haji-Abolhassani I, Ganesh S, et al. A novel wearable device for continuous temperature monitoring & fever detection. IEEE J Transl Eng Health Med. 2021;9:2700407. doi:10.1109/JTEHM.2021.3098127
- Offodile AC II, Delgado D, Lin YL, et al. Integration of remote symptom and biometric monitoring into the care of adult patients with cancer receiving chemotherapy—a decentralized feasibility pilot study. JCO Oncol Pract. 2023;19:e811-e821. doi:10.1200/OP.22.00676
- Jacobsen M, Gholamipoor R, Dembek TA, et al. Wearable based monitoring and self-supervised contrastive learning detect clinical complications during treatment of Hematologic malignancies. npj Digit Med. 2023;6:105. doi:10.1038/s41746-023-00847-2
- Bradley AM, Deal AM, Buie LW, Van Deventer H. Neutropenia-associated outcomes in adults with acute myeloid leukemia receiving cytarabine consolidation chemotherapy with or without granulocyte colony-stimulating factor. Pharmacotherapy. 2012;32:1070-1077. doi:10.1002/phar.1150
- Savoie ML, Nevil TJ, Song KW, et al. Shifting to outpatient management of acute myeloid leukemia: a prospective experience. Ann Oncol. 2006;17:763-768. doi:10.1093/annonc/mdl011
- Naithani R, Kumar R, Mahapatra M, et al. Early discharge from hospital after consolidation chemotherapy in acute myeloid leukemia in remission: febrile neutropenic episodes and their outcome in a resource poor setting. Haematologica. 2008;93:1416-1418. doi:10.3324/haematol.11696
- Koenig C, Ammann RA, Kuehni CE, et al. Continuous recording of vital signs with a wearable device in pediatric patients undergoing chemotherapy for cancer—an operational feasibility study. Support Care Cancer. 2021;29:5283-5292. doi:10.1007/s00520-021-06099-8
- Massengale J, Leonard K, Holstein J, et al. Bluetooth axillary temperature monitoring in outpatient autologous stem cell transplant patients. Transplant Cell Ther. 2024;30:S419. Abstract 585. doi:10.1016/j.jtct.2023.12.597
- Stuijt DG, van Doeveren EEM, Kos M, et al. Remote patient monitoring using mobile health technology in cancer care and research: patients’ views and preferences. JCO Clin Cancer Inform. 2024;8:e2400092. doi:10.1200/CCI.24.00092