Connecting Science to Practice
This study evaluates the efficacy, safety, and cost of intravenous
(IV) versus aerosolized pentamidine for Pneumocystis jirovecii
pneumonia (PJP) prophylaxis in adults with cancer at
a National Cancer Institute–designated comprehensive cancer
center. Among the patients analyzed, low PJP breakthrough
rates were observed with both formulations, although
adverse events (AEs) and associated costs were
significantly higher with aerosolized pentamidine than with
IV pentamidine. These findings show that IV pentamidine
may be a preferable alternative when trimethoprim plus sulfamethoxazole
is not tolerated, offering lower costs and improved
tolerability. This research adds information regarding
the efficacy of pentamidine for PJP prophylaxis in
addition to providing pharmacists with information on
cost-effective, patient-centered care and minimizing unnecessary
AEs in immunocompromised patients.
Pneumocystis jirovecii pneumonia (PJP) is an opportunistic lung infection, with nearly all cases occurring in immunocompromised patients.1 The National Comprehensive Cancer Network recommends PJP prophylaxis among high-risk groups, such as those receiving hematopoietic stem cell transplantation (HSCT), CAR T-cell therapy, and various treatments for acute lymphoblastic leukemia.2 Literature estimates that the incidence of PJP in patients with acute lymphoblastic leukemia ranges from 22% to 45% without prophylaxis, and approximately 25% of patients have PJP after 8 weeks of chronic high-dose steroid use without prophylaxis.1,3 In addition, patients with PJP and no HIV have a mortality rate of approximately 35% to 55% without treatment and of 10% to 20% with treatment, further emphasizing the value of prophylaxis.1,3,4
Trimethoprim plus sulfamethoxazole is the preferred prophylaxis for PJP.2 However, tolerability, hypersensitivity reactions, and adverse events (AEs), such as myelosuppression and hyperkalemia, pose significant challenges in some patients; up to 47% of patients with HIV require an alternative to trimethoprim plus sulfamethoxazole due to AEs.2,5 Pentamidine is often chosen as a second-line option because of its convenient monthly dosing schedule and favorable AE profile compared with alternative agents, including dapsone and atovaquone. Pentamidine may be administered via either aerosolized or intravenous (IV) routes.2 Historically, aerosolized pentamidine has been preferred over IV because of the high rate of AEs during treatment with IV pentamidine.3,6,7 However, administering aerosolized pentamidine has operational challenges, such as the need for a dedicated negative pressure room with trained personnel and specialized equipment.8
Previous studies that examined the use of IV or aerosolized pentamidine have noted few breakthrough cases. Five observational studies that focused specifically on the efficacy of IV pentamidine in adults after allogeneic or autologous HSCT were identified, and no breakthrough cases of PJP were noted in the combined 1151 patients.5,9-12 Among patients receiving aerosolized pentamidine for primary prophylaxis, Evernden and colleagues analyzed 649 adults who had allogeneic HSCT, 36 of which received inhaled pentamidine with 3 (8.3%) breakthrough cases13 Another cohort of 192 patients who had allogeneic HSCT received aerosolized pentamidine for a median of 4 months, and 12 patients (2.7%) had breakthrough cases of PJP.14
No studies have systematically compared the rates of breakthrough PJP between IV and aerosolized pentamidine. In addition, literature evaluating the use of pentamidine for primary PJP prophylaxis in adults is limited to patients who have had HSCT.5,9-13 In March 2020, the conducting institution switched from primarily using aerosolized pentamidine to preferentially administering pentamidine via the IV route to avoid unnecessary aerosolizing procedures during the COVID-19 pandemic. In this study, we aim to describe our experience with IV pentamidine compared with aerosolized pentamidine, including rates of breakthrough PJP, AEs associated with each route, and administration costs.
Methods
This single-center, retrospective cohort study included adults with high-risk malignancies or other conditions, such as aplastic anemia, at a single academic medical center, Huntsman Cancer Institute, Salt Lake City, between May 11, 2014, and September 30, 2023, who received at least 2 consecutive doses of either IV or aerosolized pentamidine for primary PJP prophylaxis. Two consecutive doses were selected to ensure the identification of any potential breakthrough events, including those occurring early. Restricting the analysis to patients who received only a single dose of PJP prophylaxis would limit the ability to determine whether a breakthrough event was attributable to pentamidine. Patients were excluded from the study if pentamidine was used for prophylaxis any time after an episode of PJP (ie, secondary prophylaxis), did not receive at least 2 consecutive doses of a single route, or were not treated for a condition by a provider at our institution. If patients received IV and aerosolized pentamidine during the study period, they were allocated to the treatment group in which they received the longest consecutive therapy.
For PJP prophylaxis, IV pentamidine was administered as a 4-mg/kg dose (maximum 300 mg) every 28 days. To optimize the tolerability of IV pentamidine, our institution added cetirizine 10 mg as a premedication and increased the infusion time to a minimum of 90 minutes in December 2020. For aerosolized pentamidine, the dose was 300 mg inhaled every 28 days. Patients who received any pentamidine doses were identified via the electronic data warehouse and manual data were extracted via chart review, which included the confirmation of inclusion and exclusion criteria.
Three major analyses for each route of pentamidine were performed, including the rates of breakthrough PJP, incidence of AEs, and cost of administration. Breakthrough PJP cases were analyzed with IV versus aerosolized pentamidine. To account for limitations of retrospective differentiation of PJP colonization versus PJP that caused true infection, 2 definitions of breakthrough were employed. First, a breakthrough PJP test was defined as a positive PJP direct fluorescence assay or PJP polymerase chain reaction at least 7 days after the first qualifying dose of pentamidine and no later than 28 days after the last qualifying dose, in line with previous studies that examined PJP breakthrough cases.5,9,10 Because positive tests may reflect colonization and not true disease, we also evaluated patients with a positive PJP diagnosis based on clinical criteria to provide a more specific estimate of breakthrough infection. A manual chart review was performed for the evaluation of symptoms, laboratory results, imaging, and consultations with infectious disease physician notes to determine whether colonization or infection was clinically suspected. Cases were further classified as possible, probable, or proven disease using the European Organisation for Research and Treatment of Cancer/Mycoses Study Group Education and Research Consortium (EORTC/MSGERC) consensus definitions.15
To compare the rates of AEs, we randomly selected and analyzed 100 patients per administration route. Each encounter associated with the first dose was evaluated for symptoms through a review of the nursing notes. The medication administration record was reviewed for additional medications given for symptom management and whether the rate of infusion was slowed or stopped.
Cost estimates of medications, supplies, and staff requirements were used to determine the cost per dose. For medications and supplies needed, the wholesale acquisition cost was used, and the average hourly salary in the conducting state for either nurse or respiratory therapist (as applicable) were used for the cost estimate.
Statistical Analysis
Descriptive statistics were used to analyze the patients’ demographic information. The sample size was calculated using historical breakthrough rates of 1% for IV pentamidine and 3% for aerosolized pentamidine.5,9-13 The estimated sample size to detect a 2% difference between the groups using a 1-sided alpha of 0.05 and 80% power was 1600 patients (800 in each group). However, we ultimately examined all patients who had met our inclusion criteria and who were identified since our institution adopted our electronic medical record. A log-rank test was used to compare the rate of breakthrough between the 2 groups. Because the event rate was so low, we did not perform a multivariable regression.
Results
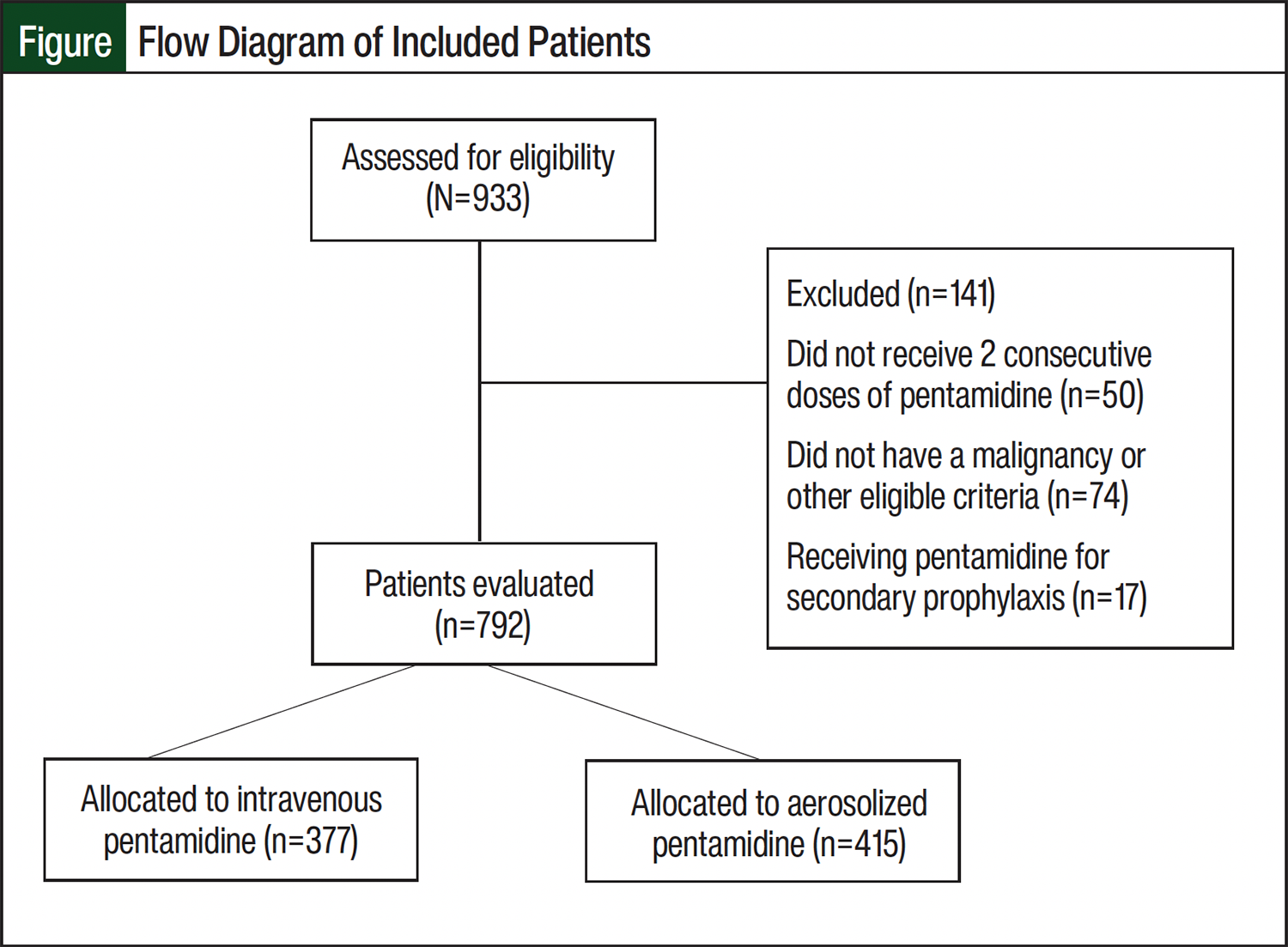
A total of 933 patients who received either IV or aerosolized pentamidine at the conducting institution during the study period were identified. After the exclusion criteria were applied, 792 patients remained eligible for analysis, with 377 in the IV group and 415 in the aerosolized group (Figure). The vast majority of doses received after 2020 were administered via the IV route (Appendix Figure S1).
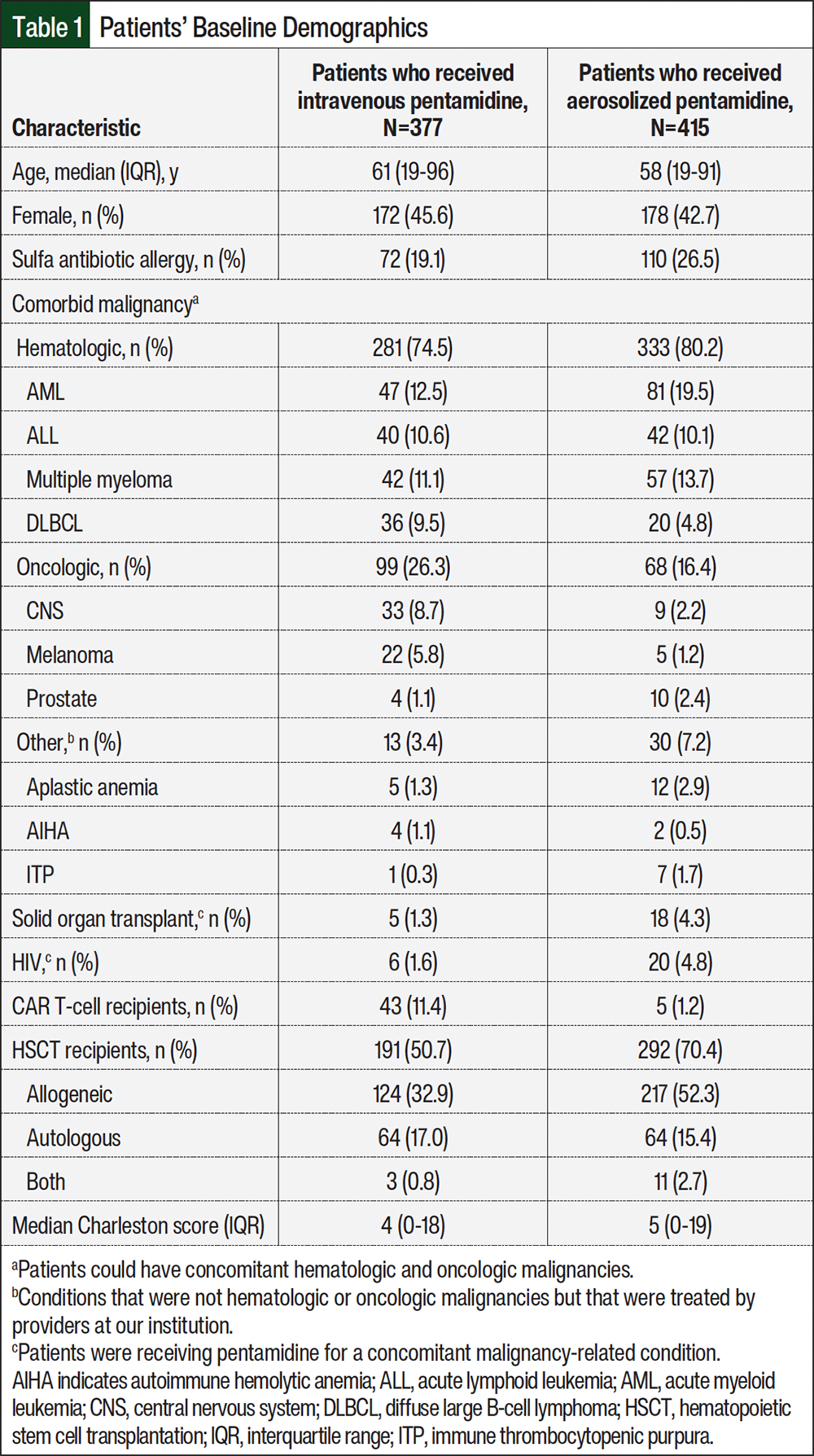
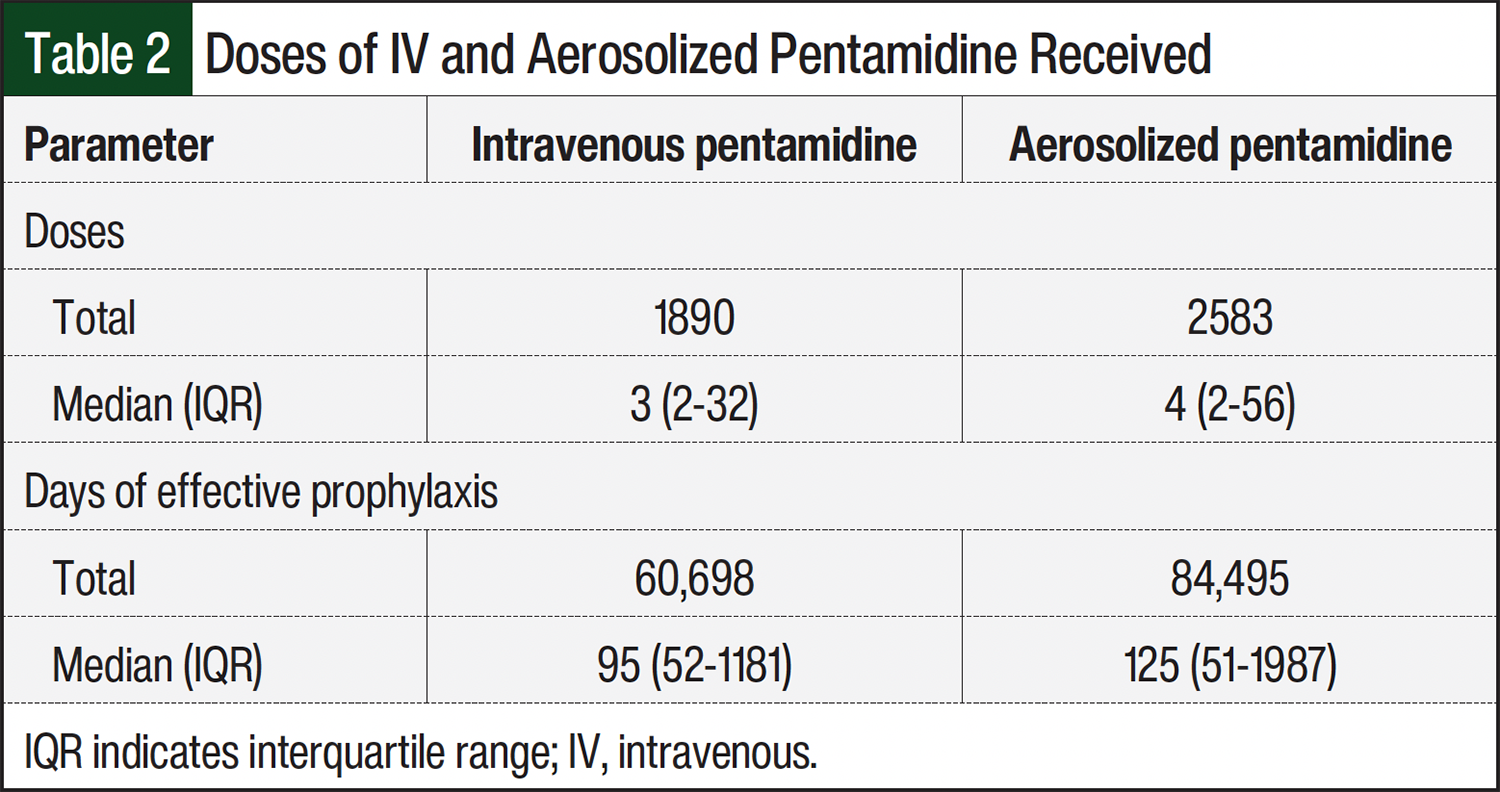
Overall, the baseline characteristics between the IV and aerosolized groups were balanced (Table 1). HSCT recipients represented 61% (n=483) of the study population. For prophylaxis, 1890 doses of IV pentamidine were administered to 377 patients, with a median of 3 doses per patient. Conversely, 2583 doses of aerosolized pentamidine were administered to 415 patients, with a median of 4 doses per patient (Table 2).
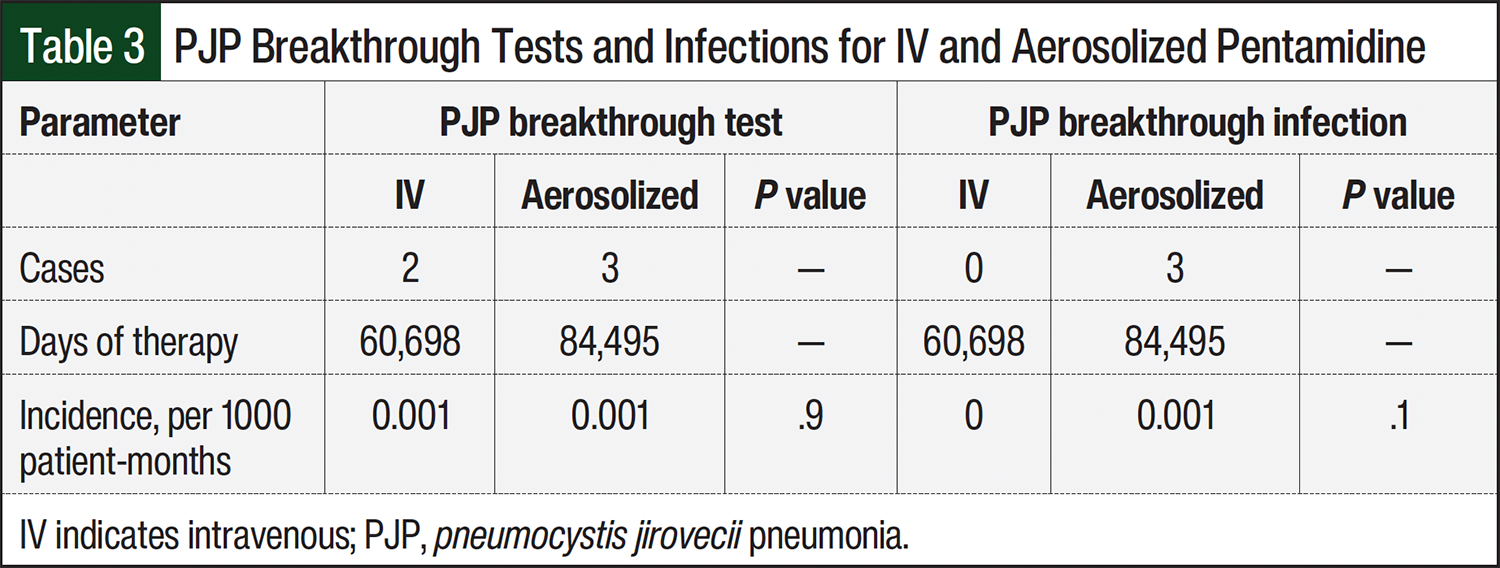
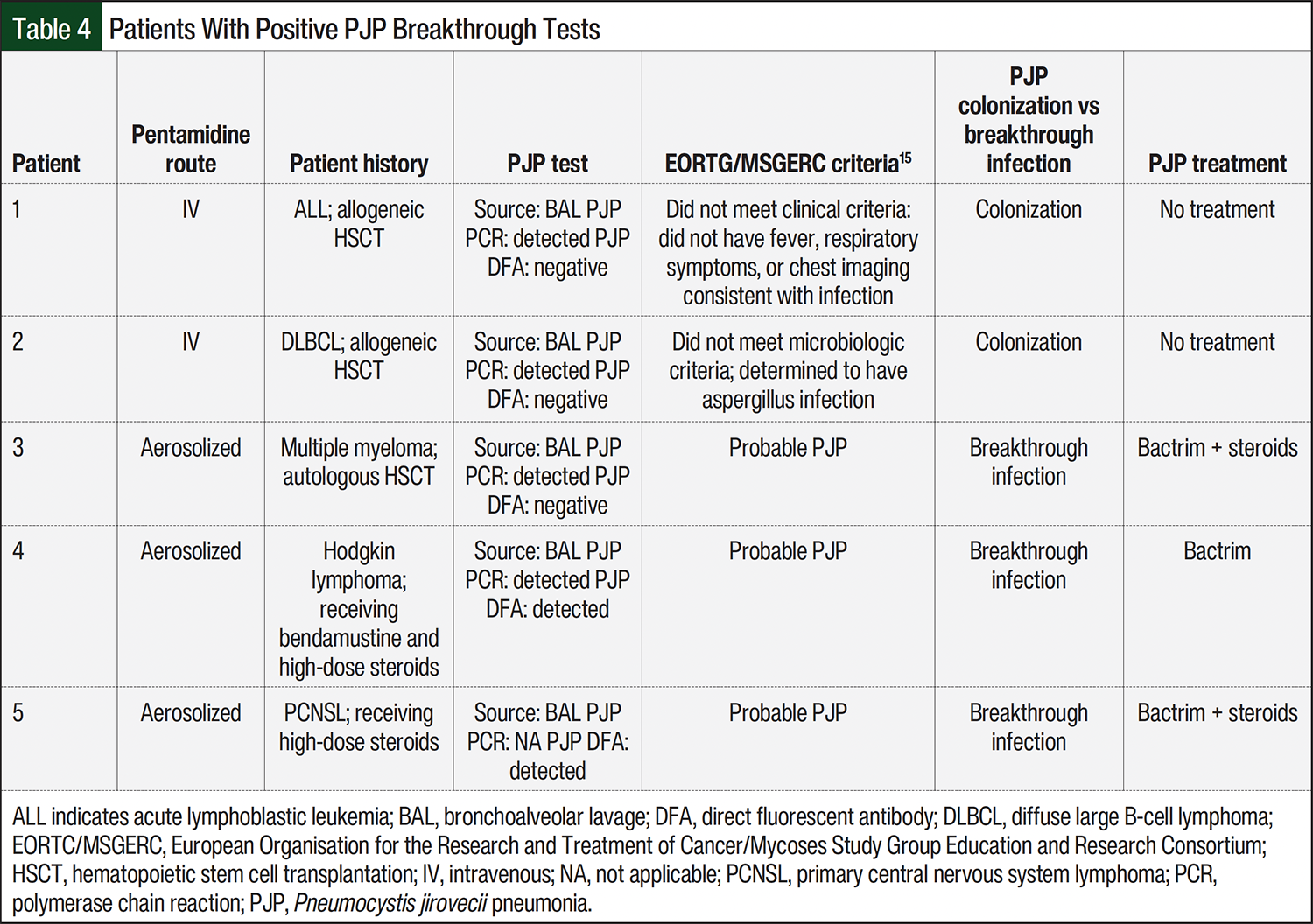
Five positive breakthrough PJP tests were identified, 2 in the IV and 3 in the aerosolized group. The incidence rate of PJP breakthrough tests in both groups was 0.001 per 1000 patient months (Table 3). Based on manual review, the 2 patients in the IV pentamidine group had positive tests that were determined to be colonization, as stated in the infectious disease physician’s note. Because these patients did not meet the EORTG/MSGERC criteria for PJP infection, they did not receive treatment for PJP. The 3 patients in the aerosolized pentamidine group were determined to have probable PJP infections per the EORTG/MSGERC criteria and received treatment for PJP infection (Table 4).15 Therefore, the incidence rate for PJP breakthrough disease in the IV group was 0 compared with 0.001 per 1000 patient months in the aerosolized group (Table 3).
Among 100 selected patients who received IV pentamidine, 11 (11%) had documented AEs, most frequently phlebitis, abdominal cramping, and nausea/vomiting. Two patients required additional medications for symptom management (nausea). In accordance with our protocol, 80 of these 100 patients received cetirizine as a premedication. The most common starting infusion rate was 90 minutes (Table 5). There were no cases of acute kidney injury attributed to pentamidine infusions, and none of the patients required hospital admission or a visit to urgent care.
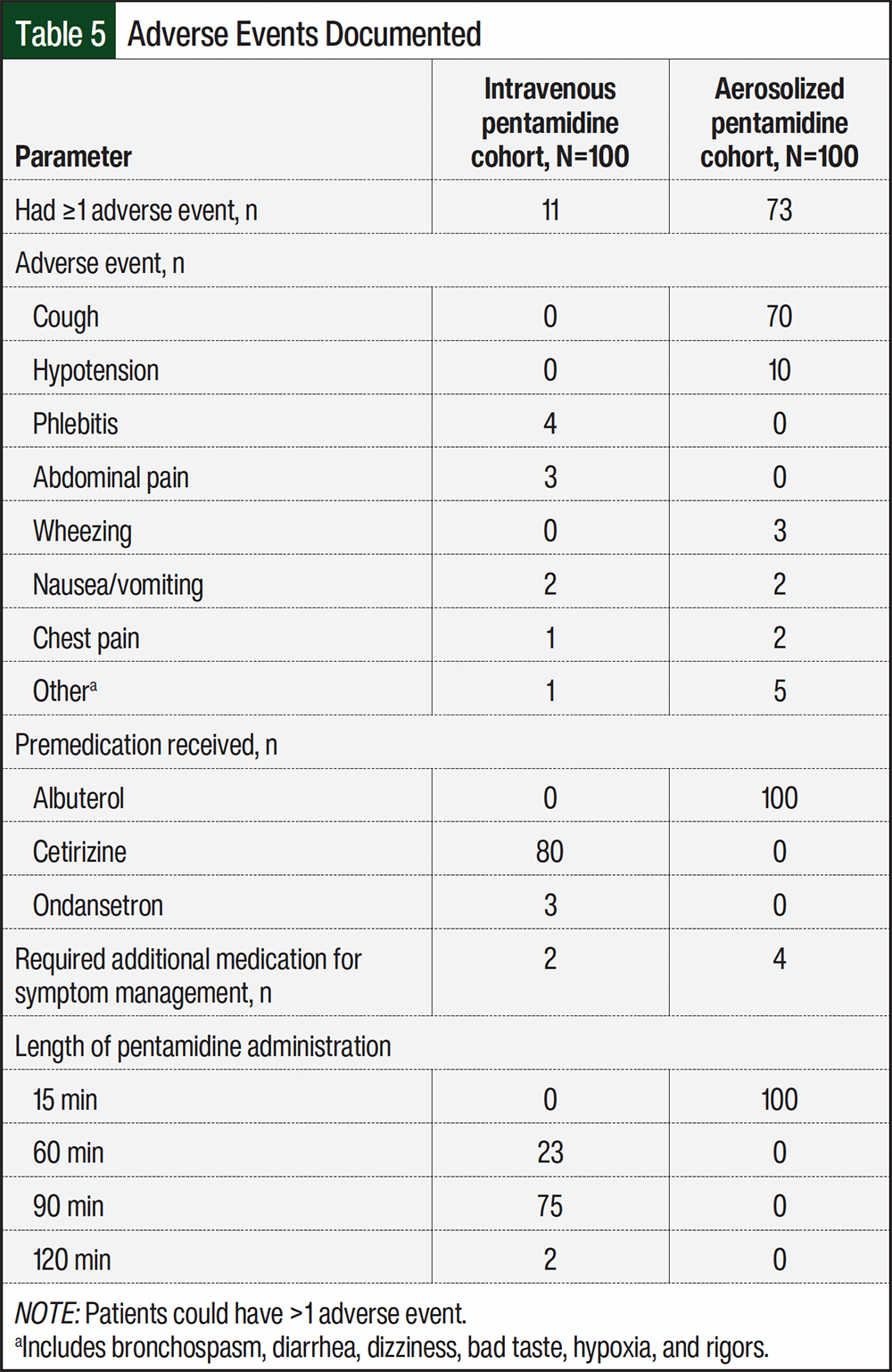
For the selected 100 patients who received aerosolized pentamidine, 73 (73%) had documented AEs, most frequently cough, hypotension, and bronchospasm. Of the 73 patients, 4 (5.5%) required additional medications for symptom management, primarily rescue albuterol. All of the patients received albuterol as a premedication and were given a dose of 300 mg at a rate of 24 mL/hr (Table 5).
The estimated cost per dose of the IV pentamidine was $131.47, which is markedly lower than the $249.54 estimated for the aerosolized formulation. The main cost difference between the formulations was the wholesale acquisition cost of the pentamidine vials. The cost per vial for the IV formulation was $112.50 compared with $200.27 for the aerosolized formulation. Additional unique expenses associated with the aerosolized formulation include N95 masks ($15.75), Respirgard II ($5.62), and respiratory therapists ($58.46 per hour).
Discussion
In this retrospective, single-center study, very low breakthrough rates of PJP were identified for the IV and aerosolized pentamidine groups, similar to previous studies that evaluated patients who received each medication route.5,9-14 Trimethoprim plus sulfamethoxazole remains the drug of choice for PJP prophylaxis in immunocompromised hosts because of low rates of breakthrough PJP (<0.5%) and extensive supporting literature.2,4 However, trimethoprim plus sulfamethoxazole–related allergies and AEs, such as hyperkalemia and thrombocytopenia, limit the use of this combination treatment in certain patients. Literature is evolving regarding the management of trimethoprim plus sulfamethoxazole–related allergy challenges and dosing alterations may assist in laboratory-related AEs.16,17 However, in the setting of true intolerances and allergies to trimethoprim plus sulfamethoxazole, pentamidine has a role in therapy for PJP prophylaxis. The low breakthrough rates of PJP with IV and aerosolized pentamidine in this study are comparable with historical breakthrough rates reported with trimethoprim plus sulfamethoxazole.18,19 Among other prophylactic options, studies report breakthrough rates up to 7.2% with dapsone, and are not well categorized for atovaquone.18,19
This study did not include dapsone or atovaquone because they are oral treatment options that patients use at home, making adherence difficult to assess. This uncertainty complicates the interpretation of breakthrough rates when comparing these agents with pentamidine formulations, whose administrations are documented in the electronic medical record. In addition, pentamidine is the preferred second-line PJP prophylaxis option at the conducting institution if trimethoprim plus sulfamethoxazole cannot be used, meaning that the number of patients who received atovaquone or dapsone at our institution would be very low in comparison.
AEs were more frequently reported in the aerosolized group (73%) compared with the IV group (11%). In addition, specific AEs reported in trials, such as a 6% rate of hypoglycemia, with IV pentamidine may not have been seen in the analysis of this study, likely because of the difference in laboratory testing, frequency of monitoring required in trials compared with real-world practice, and the use of prophylactic dosing rather than treatment dosing.7,20 Because it is not routine to check blood glucose levels after a pentamidine infusion at our institution, it is possible some patients were hypoglycemic. However, there were no symptoms of severe hypoglycemia in the nursing notes.
Most patients who received IV pentamidine were dosed after our institution added cetirizine routinely as a premedication, which may explain the low rates of reactions. In addition, the absence of hypotension in the IV pentamidine group could likely be attributed to the extended infusion time of 90 minutes. However, none of the patients in either cohort had AEs that warranted inpatient admission or a visit to urgent care.
In terms of cost, aerosolized pentamidine was almost double the cost of the IV formulation. The primary driver of this cost difference was the variance in the cost of pentamidine vials, because distinct vial drugs are used for the IV and inhaled formulations at our institution to avoid medication errors. Although the contents of the vials are identical, the compounding instructions for the formulations differ. At our institution, we use the vial associated with each specific formulation to comply with the specific compounding instructions; however, this might not reflect all institutions’ practices. Specifically, the wholesale acquisition cost for the IV formulation vial is approximately $112, contrasting with the roughly $200 cost for the inhaled formulation vial. Moreover, additional expenses associated with the inhaled formulation, including the requirement for N95 masks, nebulizers, and specialized staff further contribute to the overall higher cost. Other factors that could affect the cost analysis or preferred route of administration for other institutions would be resources available, such as infusion centers for outpatient IV pentamidine or negative pressure rooms for aerosolized pentamidine, time requirements to give each formulation, shortages in staff or medication, or risk tolerance associated with aerosolizing procedures.
Limitations
Our study has limitations, including its retrospective design. This study’s data are from a single center, and the data analysis was limited by the level of detail in the patients’ charts. Our sample size was small for several reasons. We may not have identified all eligible patients, because patients could have received pentamidine or a PJP diagnosis at outside institutions. Because we required at least 2 consecutive doses of the same formulation for primary prophylaxis, fewer patients were eligible for study inclusion. Also, the time our institution has used the current electronic medical record system limited the number of patients available for analysis.
Despite these limitations, we collected and analyzed data for a diverse patient population, including a large non-HSCT group, over nearly 10 years. Another limitation was that our cost analysis was restricted to direct costs, such as medications and supplies; however, indirect costs, such as scheduling, patient transport, negative pressure room, infusion suite availability, and inpatient beds, could not be assessed and were therefore not included in the cost analysis. In addition, any potential reimbursements from insurance companies that the hospital would receive from administering this medication were not accounted for. Our findings highlight an opportunity for healthcare systems to evaluate the direct costs associated with different administration routes.
Conclusion
Although trimethoprim plus sulfamethoxazole remains the standard of care for PJP prophylaxis, IV and aerosolized pentamidine had low rates of breakthrough PJP in adults receiving care at our institution. We identified the advantages associated with IV pentamidine, including a lower cost per dose and a more favorable AE profile versus aerosolized pentamidine. Additional research should be conducted on the efficacy of IV versus aerosolized pentamidine as secondary prophylaxis.
Disclosure Statement
Dr Julian was an ad board consultant of Johnson & Johnson; Dr Jones is a consultant to KelleyCPharmD LLC and GatherEd, and is a consultant and has received honoraria from Pharmacy Times CE; Dr Imlay owns stock in Recursion Pharmaceuticals; Dr Peterson, Dr Greenlee, and Dr Ditolla have no conflicts of interest to report.
References
- Limper AH. In search of clinical factors that predict risk for Pneumocystis jirovecii pneumonia in patients without HIV/AIDS. Am J Respir Crit Care Med. 2018;198:1467-1468. doi:10.1164/rccm.201807-1358ED
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: prevention and treatment of cancer-related infections. Version 2.2025. January 22, 2026. Accessed February 17, 2026. www.nccn.org/professionals/physician_gls/pdf/infections.pdf
- Lee EH, Kim EY, Lee SH, et al. Risk factors and clinical characteristics of Pneumocystis jirovecii pneumonia in lung cancer. Sci Rep. 2019;9:2094. doi:10.1038/s41598-019-38618-3
- Ibrahim A, Chattaraj A, Iqbal Q, et al. Pneumocystis jiroveci pneumonia: a review of management in human immunodeficiency virus (HIV) and non-HIV immunocompromised patients. Avicenna J Med. 2023;13:23-34. doi:10.1055/s-0043-1764375
- Lim MJ, Stebbings A, Lim SJ, et al. IV pentamidine for primary PJP prophylaxis in adults undergoing allogeneic hematopoietic progenitor cell transplant. Bone Marrow Transplant. 2015;50:1253-1255. doi:10.1038/bmt.2015.131
- Balslev U, Nielsen TL. Adverse effects associated with intravenous pentamidine isethionate as treatment of Pneumocystis carinii pneumonia in AIDS patients. Dan Med Bull. 1992;39:366-368.
- L’age M, Arasteh K. Unwanted drug side effects with pentamidine inhalation. Med Klin (Munich). 1990;85:255-257.
- Brown KS, Reed MD, Dalal J, Makii MD. Tolerability of aerosolized versus intravenous pentamidine for Pneumocystis jirovecii pneumonia prophylaxis in immunosuppressed pediatric, adolescent, and young adult patients. J Pediatr Pharmacol Ther. 2020;25:111-116. doi:10.5863/1551-6776-25.2.111
- McCollam S, Lewis JS 2nd, Bubalo J, Diaz A. Pneumocystis jirovecii pneumonia prophylaxis with intravenous pentamidine in adult allogeneic hematopoietic stem cell transplant patients. Antimicrob Agents Chemother. 2022;66:e0083322. doi:10.1128/aac.00833-22
- Diri R, Anwer F, Yeager A, et al. Retrospective review of intravenous pentamidine for Pneumocystis pneumonia prophylaxis in allogeneic hematopoietic stem cell transplantation. Transpl Infect Dis. 2016;18:63-69. doi.org/10.1111/tid.12486
- Sweiss K, Anderson J, Wirth S, et al. A prospective study of intravenous pentamidine for PJP prophylaxis in adult patients undergoing intensive chemotherapy or hematopoietic stem cell transplant. Bone Marrow Transplant. 2018;53:300-306. doi:10.1038/s41409-017-0024-1
- Awad W, Asaad A, Al-Yasein N, Najjar R. Effectiveness and tolerability of intravenous pentamidine for Pneumocystis carinii pneumonia prophylaxis in adult hematopoietic stem cell transplant patients: a retrospective study. BMC Infect Dis. 2020;20:400. doi.org/10.1186/s12879-020-05127-y
- Evernden C, Dowhan M, Dabas R, et al. High incidence of Pneumocystis jirovecii pneumonia in allogeneic hematopoietic cell transplant recipients in the modern era. Cytotherapy. 2020;22:27-34. doi:10.1016/j.jcyt.2019.11.002
- Marras TK, Sanders K, Lipton JH, et al. Aerosolized pentamidine prophylaxis for Pneumocystis carinii pneumonia after allogeneic marrow transplantation. Transpl Infect Dis. 2002;4:66-74. doi:10.1034/j.1399-3062.2002.t01-1-00008.x
- Lagrou K, Chen S, Masur H, et al. Pneumocystis jirovecii disease: basis for the revised EORTC/MSGERC invasive fungal disease definitions in individuals without human immunodeficiency virus. Clin Infect Dis. 2021;72(suppl 2):S114-S120. doi:10.1093/cid/ciaa1805
- Krantz MS, Stone CA Jr, Abreo A, Phillips EJ. Oral challenge with trimethoprim-sulfamethoxazole in patients with “sulfa” antibiotic allergy. J Allergy Clin Immunol Pract. 2020;8:757-760.e4. doi:10.1016/j.jaip.2019.07.003
- Waldron JL, Rose M, Vogrin S, et al. Development and validation of a sulfa antibiotic allergy clinical decision rule. JAMA Netw Open. 2023;6:e2316776. doi:10.1001/jamanetworkopen.2023.16776
- Williams KM, Ahn KW, Chen M, et al. The incidence, mortality and timing of Pneumocystis jiroveci pneumonia after hematopoietic cell transplantation: a CIBMTR analysis. Bone Marrow Transplant. 2016;51:573-580. doi:10.1038/bmt.2015.316
- Chiu CY, Ching PR. Incidence of Pneumocystis pneumonia in immunocompromised patients without human immunodeficiency virus on intravenous pentamidine prophylaxis: a systematic review and meta-analysis. J Fungi (Basel). 2023;9:406. doi:10.3390/jof9040406
- Pentam (pentamidine isethionate) injection, for intravenous use [prescribing information]. Fresenius Kabi USA, LLC; May 2022. Accessed March 18, 2026. https://editor.fresenius-kabi.us/PIs/US-PH-Pentam_300_FK_45851D_May_2022-PI.pdf