Connecting Science to Practice
Crucial processes, including prehydration, the interpretation
of laboratory tests, and proper preparation of chemotherapy,
may lead to delays in the timely administration of
chemotherapy for pediatric patients in the inpatient setting.
This study identified multiple points of the inpatient chemotherapy
process at which institutions may experience the
greatest delays. These are not robust data on this area of pediatric
oncology practice, and this study highlights opportunities
for improvement as well as demonstrates the potential
impact of implementing practices, such as a rapid hydration
protocol, to reduce time from admission to chemotherapy
initiation.
Administering chemotherapy in the inpatient setting can place a logistical burden on healthcare workers, patients, and caregivers, but it is necessary in a variety of circumstances. There are specific groups of pediatric patients requiring chemotherapy administration in the inpatient setting, including patients with a high risk for tumor lysis syndrome, patients receiving chemotherapy agents with a high risk for adverse events that require stringent monitoring, and patients hospitalized for other reasons who are due to receive chemotherapy per their treatment regimen.1 Chemotherapy agents, such as cisplatin, cyclophosphamide, ifosfamide, and methotrexate, pose a risk for nephrotoxicity, and it is pertinent for patients to receive proper intravenous (IV) hydration before administration.2 Protocols that include anthracycline agents, such as doxorubicin and daunorubicin, incorporate echocardiograms to monitor for cardiotoxicity.3 Important considerations before administering chemotherapy include prehydration, timely interpretation of laboratory values and monitoring tests, and proper handling and preparation of chemotherapy.
Although these processes are crucial to ensuring safe chemotherapy administration, delays can impact patients’ length of stay and overall satisfaction with care.4-9 Prolonged length of stay is related to increased risk for hospital-associated conditions, such as thrombosis and infections.5 Improving overall workflow is crucial to ensuring the timely administration of inpatient chemotherapy, reducing hospital length of stay and institutional costs, and increasing patient and caregiver satisfaction.10 Identified workflow improvements implemented in the outpatient setting may reduce time to inpatient chemotherapy initiation, such as outpatient laboratory monitoring, signing chemotherapy orders before admission, and urinary alkalinization before admission.7 Interdisciplinary collaboration is necessary to ensure the prompt and safe administration of chemotherapy for pediatric patients in the inpatient setting.
A medication use evaluation completed at our institution in 2024 examined hydration fluids in pediatric patients receiving select chemotherapy regimens and showed that the mean time between starting IV fluids and chemotherapy administration was 7.76 hours. These results helped establish a protocol for rapid hydration with the aim of shortening the time to the administration of chemotherapy for patients requiring prehydration. The purpose of this study is to assess the potential barriers to initiating chemotherapy for pediatric patients in the inpatient setting, including evaluating the impact of a recently implemented protocol for rapid hydration before chemotherapy.
Methods
A single-center, retrospective study was performed using electronic health records (EHRs) to evaluate the barriers to the timely initiation of inpatient chemotherapy for pediatric patients. This retrospective review also included an evaluation of the time to the administration of chemotherapy for pediatric patients receiving IV hydration based on an institutional rapid hydration protocol implemented in June 2024. The study was conducted in patients admitted to the inpatient oncology unit at a freestanding children’s hospital from July 1, 2024, to December 31, 2024. The local investigational review board and the Office of Research Administration approved this study.
Patients admitted to the pediatric oncology unit to receive inpatient chemotherapy were included in the study. Patients newly diagnosed with a malignancy who initiated chemotherapy during the same admission and patients who were not admitted on the day their chemotherapy was due were excluded from this study. At our institution, there are a couple of different approaches for admitting patients to receive chemotherapy. Patients needing procedures such as a lumbar puncture for intrathecal chemotherapy administration are admitted the evening before starting chemotherapy to obtain the necessary laboratory monitoring and to ensure that they are adequately hydrated. Patients who do not require sedation services on admission arrive in our outpatient clinic in the morning to obtain a point-of-care complete blood count. If they meet the platelet and neutrophil thresholds necessary to receive chemotherapy, they will be admitted to the oncology unit, where organ function laboratory monitoring is checked, and they receive hydration fluids as well as any necessary supportive care medications. Patients may also require other monitoring procedures, such as an echocardiogram, on inpatient admission. Once patients meet all criteria for treatment, an oncology provider will place an ok-to-treat order indicating that it is safe to proceed with chemotherapy. The hospital pharmacy then prepares and delivers the chemotherapy, and it is checked by 2 oncology-trained nurses before administration.
Data collection includes the time and date of admission; time of laboratory test order release, collection, and results; time of echocardiogram completion and interpretation; presence of provider signatures for chemotherapy; time of chemotherapy order release; time of chemotherapy verification in the EHR by a pharmacist; and time of chemotherapy initiation. Additional data points collected for patients receiving the rapid hydration protocol included the time of rapid hydration fluid order release and initiation, rate of IV fluid administration, name and dose of the chemotherapy agent, urine-specific gravity readings, time-to-goal-specific gravity per protocol, and urine pH readings for patients receiving IV methotrexate. Additional data were collected to assess the pharmacy medication preparation time. These data points included the time the drug was entered in the preparation queue, time of preparation completion, time of drug verification by a pharmacist, and time the drug preparation was completed.
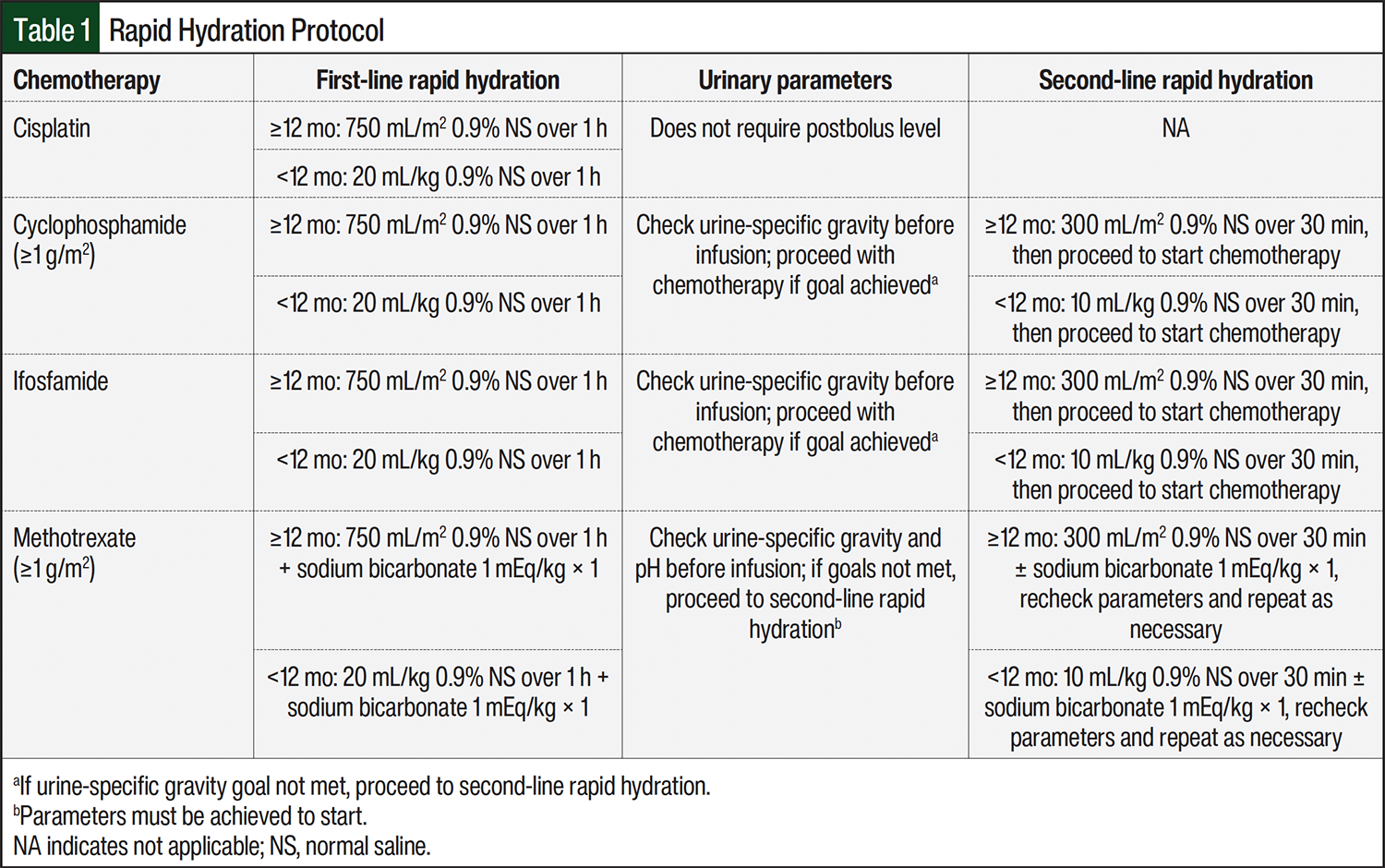
The rapid hydration protocol at our institution aims to optimize the patient’s hydration status before the administration of certain chemotherapy agents. Agents requiring rapid hydration per the protocol include cisplatin, cyclophosphamide doses ≥1 g/m2, ifosfamide, and methotrexate doses ≥1 g/m2. Patients and their caregivers are instructed to increase fluid intake before the scheduled inpatient admission for chemotherapy. Urine-specific gravity readings are obtained for all patients on admission, and urine pH readings are obtained for all patients receiving methotrexate. The goal urine-specific gravity is ≤1.01 and the goal urine pH for patients receiving methotrexate is ≥7. Patients receiving cisplatin, cyclophosphamide ≥1 g/m2, or ifosfamide receive an initial IV fluid bolus of 750 mL/m2 of 0.9% sodium chloride over 1 hour if aged ≥12 months or 20 mL/kg over 1 hour if aged <12 months. This protocol does not require an additional IV fluid bolus for patients receiving cisplatin who do not meet the urinary parameters after the initial bolus.
Patients receiving cyclophosphamide ≥1 g/m2 or ifosfamide who do not meet the urinary parameters after the initial IV fluid bolus will receive an additional IV fluid bolus of 300 mL/m2 of 0.9% sodium chloride over 30 minutes if aged ≥12 months or 10 mL/kg over 30 minutes if aged <12 months before proceeding with chemotherapy. Patients receiving methotrexate ≥1 g/m2 receive an initial IV fluid bolus of 750 mL/m2 0.9% sodium chloride over 1 hour if aged ≥12 months or 20 mL/kg over 1 hour if aged <12 months plus a 1-mEq/kg dose of IV sodium bicarbonate for urinary alkalization. If these patients do not meet urine pH and specific gravity requirements, they receive additional IV fluid boluses of 300 mL/m2 of 0.9% sodium chloride over 30 minutes if aged ≥12 months or 10 mL/kg over 30 minutes if aged <12 months, plus 1-mEq/kg doses of IV sodium bicarbonate if needed until these parameters are met. Patients receiving methotrexate are required to meet the urinary parameters before initiating chemotherapy. The rapid hydration protocol procedures for each chemotherapy agent are summarized in Table 1.
The primary objective of this study was to identify and assess potential barriers to the timely administration of chemotherapy in the inpatient setting for pediatric patients. The secondary objective was to evaluate the time to administration of inpatient chemotherapy after the initiation of fluids in accordance with the rapid hydration protocol compared with preprotocol implementation. Data for these objectives were analyzed using descriptive statistics. P values were calculated from the median values using the Mann-Whitney U test.
Results
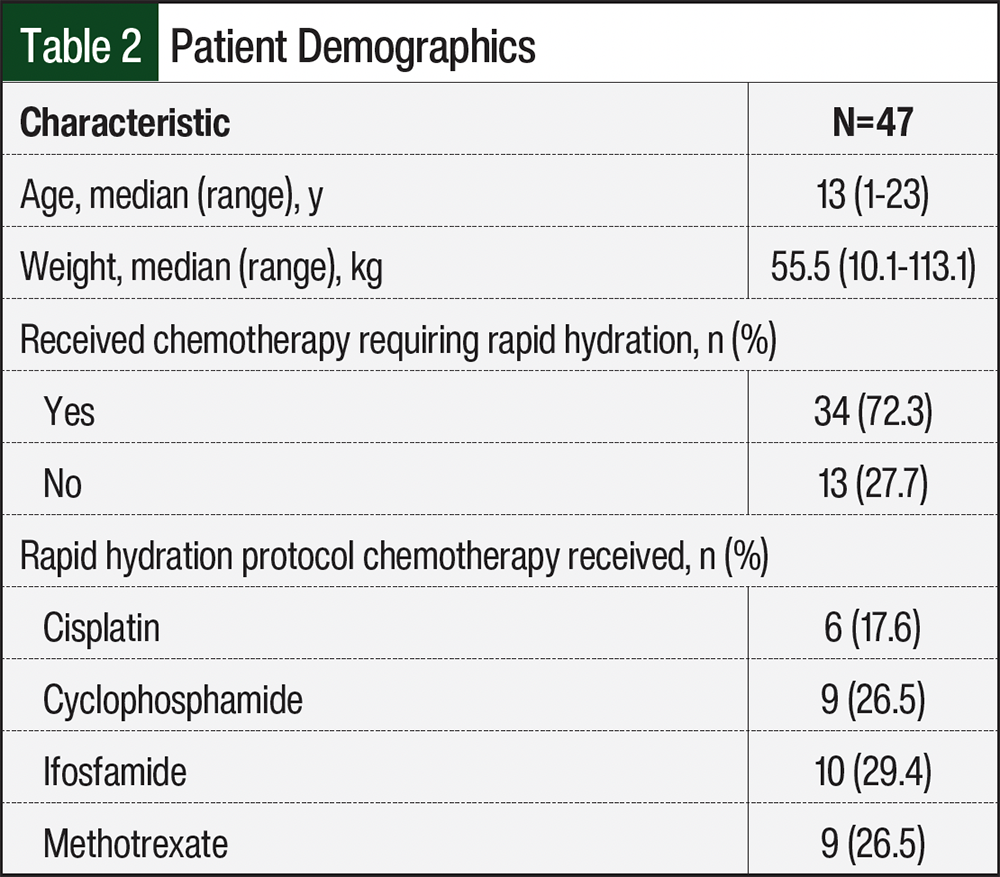
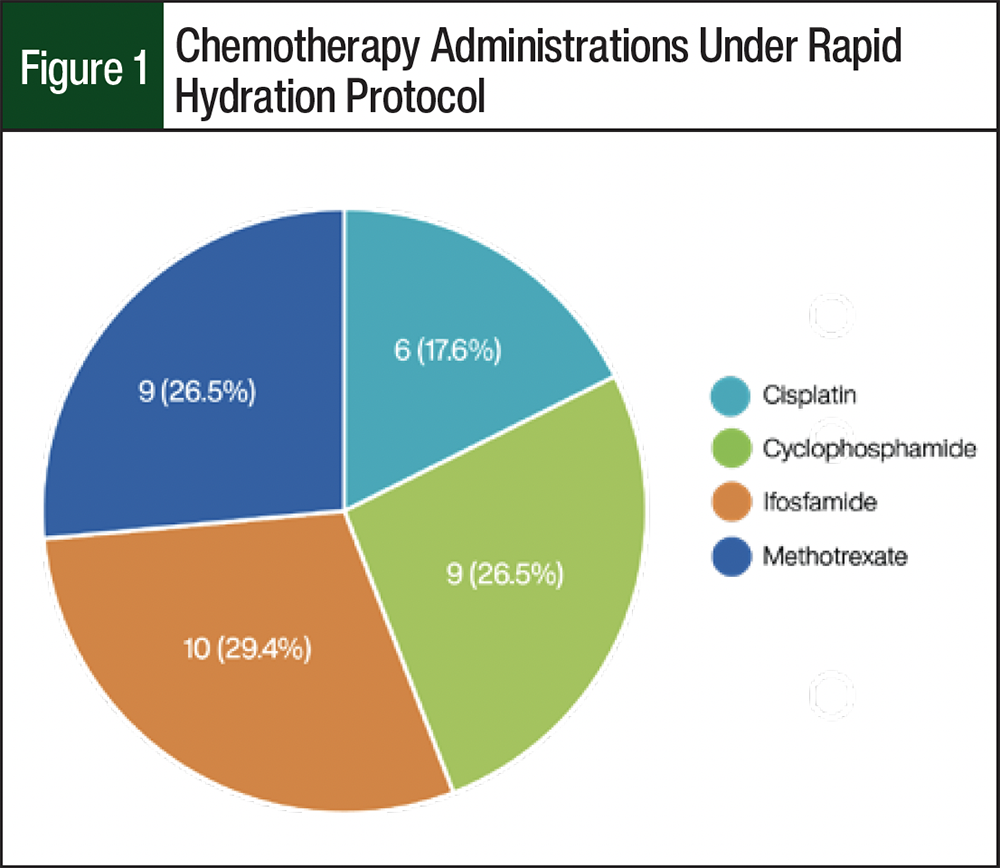
A total of 120 patients received inpatient chemotherapy during the study period, and 47 patients met the study’s inclusion criteria. Of these 47 patients, 34 patients received chemotherapy agents requiring rapid hydration per the protocol and were included in the secondary objective analysis. The patients’ demographics are shown in Table 2. The median patient age was 13 years (range, 1-23 years) and the median patient weight was 55.5 kg (range, 10.1-113.1 kg). Among the patients who received chemotherapy agents and required rapid hydration, 10 (29.4%) patients received ifosfamide, 9 (26.5%) received methotrexate (≥1 g/m2 per dose), 9 (26.5%) received cyclophosphamide (≥1 g/m2 per dose), and 6 (17.6%) received cisplatin (Figure 1).
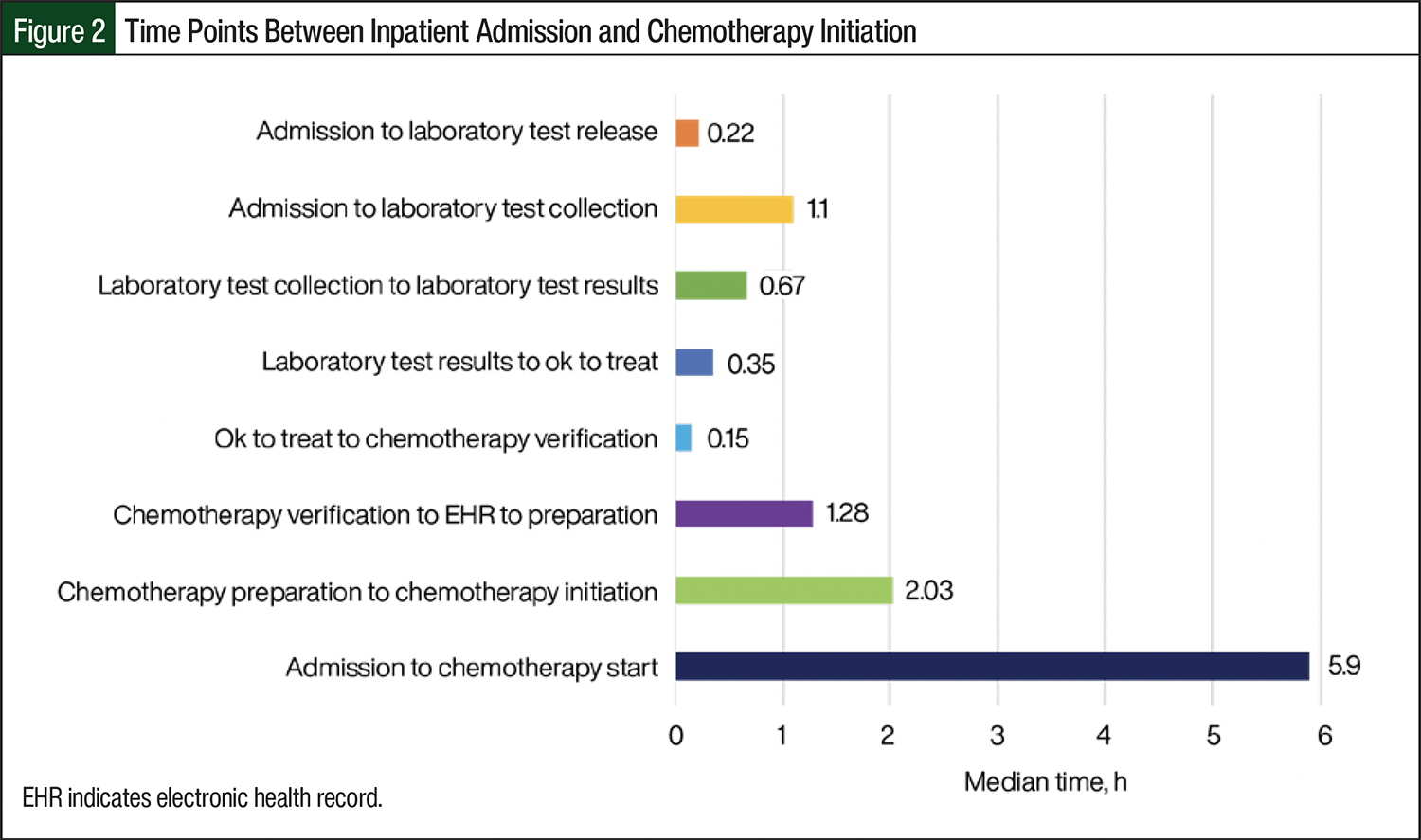
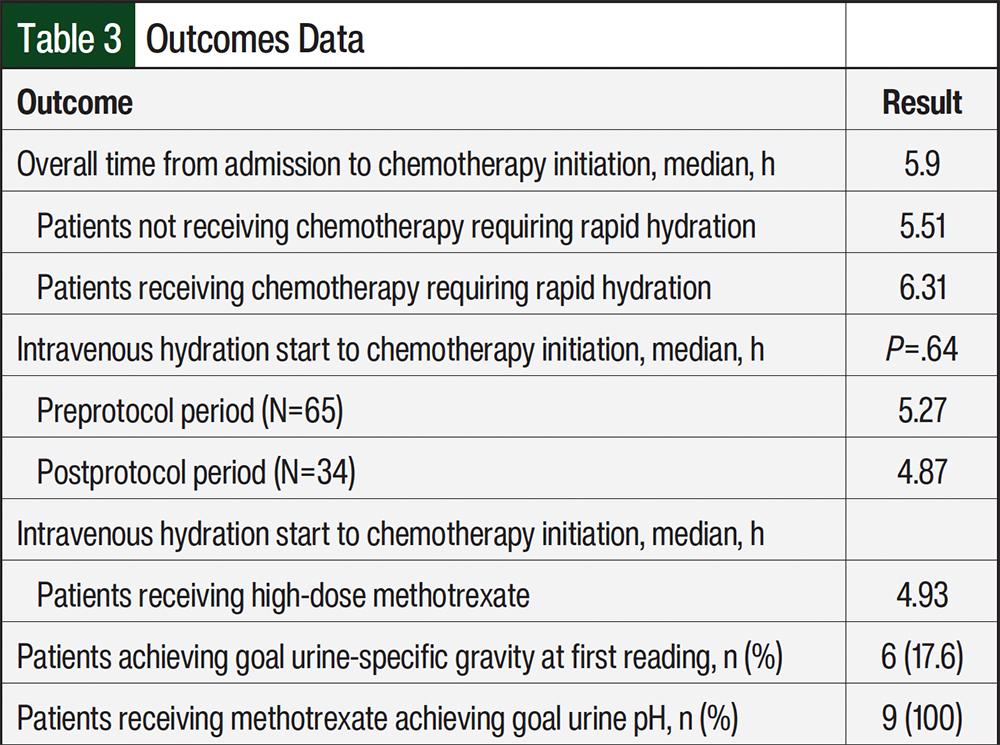
The median time from inpatient admission to chemotherapy initiation was 5.9 hours in the primary study population. For patients not requiring rapid hydration (n=13) and patients requiring rapid hydration (n=34), the median times from inpatient admission to chemotherapy initiation were 5.51 hours and 6.31 hours, respectively. Figure 2 depicts the median time points collected between inpatient admission and chemotherapy initiation for the primary analysis. For the median time points regarding laboratory processing, the time from admission to laboratory test release was 0.22 hours, the time from admission to laboratory test collection was 1.1 hours, the time from laboratory test collection to laboratory test results was 0.67 hours, and the time from laboratory results to ok to treat was 0.35 hours. For the median time points regarding pharmacy workflow, the time from ok to treat to chemotherapy verification was 0.15 hours, and the time from chemotherapy verification in the Epic EHR to chemotherapy preparation from the clean room was 1.28 hours. Last, the median time from chemotherapy preparation to initiation was 2.03 hours.
All chemotherapy orders were signed by 2 providers and were subsequently reviewed by a pharmacist before patient admission. Of note, the time points for echocardiogram performance and interpretation were also collected. There was 1 patient for whom an echocardiogram was performed and interpreted during their chemotherapy admission. The time from echocardiogram performance to interpretation was 1.48 hours.
The median time from the start of IV hydration to chemotherapy initiation in this population was compared with the preprotocol period (Table 3). The median time from the start of IV hydration to chemotherapy initiation in the preprotocol period was 5.27 hours compared with 4.87 hours in the postprotocol period (P=.64). The median time from the start of IV hydration to chemotherapy initiation for patients receiving high-dose methotrexate was 4.93 hours compared with 4.83 hours for patients requiring rapid hydration who did not receive methotrexate. All patients in this population receiving methotrexate achieved a goal urine pH of ≥7 with the first recorded urine pH. For patients receiving agents and required rapid hydration, there were 6 (17.6%) patients who achieved a urine-specific gravity goal per the protocol with the first urine-specific gravity reading. The median time to the goal-specific gravity for these patients was 2.18 hours.
Discussion
Overall, most patients at the institution initiate chemotherapy within 6 hours from their admission time. Patients receiving chemotherapy agents who require the use of the rapid hydration protocol have a slightly longer time from admission to chemotherapy initiation. This study aimed to identify and assess the barriers to initiating chemotherapy for pediatric patients in the inpatient setting. There were multiple time points identified as opportunities to decrease the time to chemotherapy initiation.
First, the median time from admission to laboratory test collection was 1.1 hours. This time could be optimized by creating a plan with the admission team and nursing staff to eliminate unnecessary wait times before laboratory test collection. Helping nursing staff promptly obtain laboratory tests by immediately releasing laboratory orders on admission and quickly sending the patient to their designated room would allow for test collection within 1 hour of admission. Alternatively, all laboratory monitoring could be obtained in an outpatient clinic before admission to help decrease time from admission to chemotherapy initiation.
A second time point identified for improvement was the time from chemotherapy verification in the Epic EHR to the preparation from the pharmacy clean room (median, 1.28 hours). This presents an opportunity for the streamlining of pharmacy workflow to ensure that there is no delay with chemotherapy agents exiting the clean room for delivery to the floor.
The time point with the greatest opportunity for improvement is the time from chemotherapy preparation to chemotherapy initiation (median, 2.03 hours). There are various possible reasons for delays at this time point, including potential delays with chemotherapy delivery to the floor from the pharmacy; delays with nursing staff retrieving chemotherapy from the medication room; unforeseen logistic issues, such as line problems; and required urinary parameters for high-dose methotrexate. Now that these time points for improvement are identified, the pharmacy, nursing, and provider staff can work to address these delays and further decrease the time to inpatient chemotherapy initiation. In addition, imaging studies, such as echocardiograms, do not greatly impact the time from admission to chemotherapy initiation, considering only 1 patient in this study had an echocardiogram reading and interpretation during their chemotherapy admission.
The secondary objective of this study was to evaluate the time to the administration of inpatient chemotherapy after the initiation of IV rapid hydration protocol fluids compared with preprotocol implementation. Before this study, our institution completed an evaluation examining hydration fluids in pediatric patients undergoing inpatient chemotherapy. This study shows a nonsignificant reduction in time from IV hydration start to chemotherapy initiation between the preprotocol and postprotocol periods (5.27 hours vs 4.87 hours, respectively; P=.64). There were 65 patients included in the preprotocol period and only 34 patients included in the postprotocol period, which could explain the lack of statistical significance for this comparison. A future study with a larger sample size could further evaluate the full impact of the rapid hydration protocol.
The median time from starting IV hydration to chemotherapy initiation among patients receiving methotrexate was similar to the overall secondary objective analysis population; therefore, there was no major delay in starting chemotherapy as a result of not meeting the urinary parameters. Urine-specific gravity and urine pH for high-dose methotrexate were assessed per protocol for patients requiring rapid hydration. The urine-specific gravity goal was ≤1.01 and the goal urine pH for methotrexate was ≥7. Patients receiving cyclophosphamide or ifosfamide who did not meet the urine-specific gravity goals after the initial IV fluid bolus received an additional IV fluid bolus over 30 minutes and then initiated chemotherapy. Also, patients receiving methotrexate were required to achieve a urine pH and urine-specific gravity goals before initiating treatment.
Limitations
This study has some limitations, including a small sample size for primary and secondary objective analyses. In addition, this was a retrospective study, which may have limited the investigators’ collected data for analysis because of potential documentation issues in the EHR.
Conclusion
Overall, optimizing the time from chemotherapy preparation to chemotherapy initiation could make the largest impact on decreasing the time from admission to chemotherapy initiation. Although the rapid hydration protocol demonstrated some improvement in chemotherapy start times, it was a nonsignificant reduction. Future projects with a larger sample size could further evaluate the full impact of this protocol. Future directions will involve working with nursing and provider staff to address identified areas for further improvement of the timely initiation of inpatient chemotherapy at our institution.
Disclosure Statement
Dr Ensor, Dr Elder, Dr Harwood, and Dr Holsteen have no disclosures to report.
References
- Dollinger M. Guidelines for hospitalization for chemotherapy. Oncologist. 1996;1:107-111.
- McKinnon K, Tran T, Lewis V. Evaluation of a pediatric pre-chemotherapy rapid hydration protocol: a quality assurance project. J Oncol Pharm Pract. 2023;29:679-684. doi:10.1177/10781552221078207
- Qiu Y, Jiang P, Huang Y. Anthracycline-induced cardiotoxicity: mechanisms, monitoring, and prevention. Front Cardiovasc Med. 2023;10:1242596. doi:10.3389/fcvm.2023.1242596
- Gupta A, Li J, Tawfik B, et al. Reducing wait time between admission and chemotherapy initiation. J Oncol Pract. 2018;14:e316-e323. doi:10.1200/JOP.17.00028
- Accordino MK, Wright JD, Vasan S, et al. Factors and costs associated with delay in treatment initiation and prolonged length of stay with inpatient EPOCH chemotherapy in patients with hematologic malignancies. Cancer Invest. 2017;35:202-214. doi:10.1080/07357907.2016.1276186
- Clarke A. Why are we trying to reduce length of stay? Evaluation of the costs and benefits of reducing time in hospital must start from the objectives that govern change. Qual Health Care. 1996;5:172-179. doi:10.1136/qshc.5.3.172
- Galeas JN, Packer S, Browne R, et al. Decreasing time to initiation of chemotherapy for patients electively admitted to a hematologic malignancy service. J Oncol Pract. 2019;15:e906-e915. doi:10.1200/JOP.19.00120
- Soh TI, Tan YS, Hairom Z, et al. Improving wait times for elective chemotherapy through pre-preparation: a quality-improvement project at the National University Cancer Institute of Singapore. J Oncol Pract. 2015;11:e89-e94. doi:10.1200/JOP.2014.000356
- Sandoval GA, Brown AD, Sullivan T, Green E. Factors that influence cancer patients’ overall perceptions of the quality of care. Int J Qual Health Care. 2006;18:266-274. doi:10.1093/intqhc/mzl014
- Nguyen TV, Ononogbu OJ, Egwim OU, et al. Reducing chemotherapy administration time on an inpatient oncology unit. J Oncol Pharm Pract. 2021;27:1878-1882. doi:10.1177/1078155220971737