Connecting Science to Practice
Patients with acute myeloid leukemia (AML) who receive
low-intensity induction therapy, such as hypomethylating
agents (azacitidine or decitabine) plus venetoclax, often
have prolonged neutropenia, which increases their infection
risk and length of hospitalization. Granulocyte colony-
stimulating factor (G-CSF) is frequently used to support
neutrophil recovery, but its use in AML remains
controversial due to concerns for disease progression. In
patients with a hypoplastic bone marrow and no evidence
of disease after induction, G-CSF may offer clinical benefit
without compromising safety. This retrospective, single-
center, cohort study evaluated G-CSF use in this specific
population to better understand its effectiveness,
safety, and financial characteristics. The findings help
clarify the use of G-CSF for patients with AML who have
a hypoplastic bone marrow and no evidence of disease,
supporting providers and pharmacists in making treatment
decisions that optimize supportive care and potentially
improve neutrophil recovery.
Acute myeloid leukemia (AML) is a hematologic malignancy that is characterized by a leukemic clone of myeloid blasts. Treatment for AML is separated into induction and consolidation therapy with the goal of obtaining complete remission (CR) and achieving durable disease control. Low-intensity induction therapy is recommended in patients who are unfit for intensive therapy.1 Patients who are likely to be unfit for intensive therapies include those with poor performance or functional status and/or older individuals with comorbid conditions.1 One of the first-line therapies for low-intensity induction includes a combination regimen with a hypomethylating agent (HMA), such as azacitidine or decitabine, plus venetoclax.1 HMA plus venetoclax therapy has synergistic activity against AML cells in vitro and an antitumorigenic benefit in vivo leading to AML cell death.2 This synergistic activity results in robust responses to low-intensity induction.2
The VIALE-A trial compared azacitidine plus venetoclax versus azacitidine plus placebo (ie, the control group). The median overall survival was higher at 14.7 months in the combination azacitidine and venetoclax group compared with 9.6 months in the control group (hazard ratio, 0.66; P<.001). In addition, the incidence of CR was higher in the combination group than in the control group (36.7% vs 17.9%, respectively; P<.001).3 With this combination regimen, patients who previously had a poor prognosis due to ineligibility for intensive induction now have an effective, lower-intensity treatment option.
The VIALE-A trial demonstrated that treatment with HMA plus venetoclax resulted in prolonged cytopenias leading to grade 3 neutropenia and grade 3 febrile neutropenia in 42% of the patients in the combination azacitidine and venetoclax group. In many patients with malignancies, granulocyte colony-stimulating factor (G-CSF) is used in those with neutropenia to encourage absolute neutrophil count (ANC) recovery and potentially prevent infection-related complications associated with reduced ANC. G-CSF accomplishes this through binding with the G-CSF receptor on the surface of myeloid cells, stimulating the production of mature neutrophils.4 As a result of this mechanism, there are concerns about the use of G-CSF in AML because of the possibility of increasing the number of malignant leukemic cells in uncontrolled disease or in patients who have not yet reached a confirmed CR. However, for patients who are in CR (defined as blasts <5% on postremission bone marrow biopsy), G-CSF may pose an opportunity to aid in count recovery without the concern for disease progression, thereby potentially decreasing the hospital length of stay and infection risks. Patients who are not yet deemed to be in CR but who have hypoplastic bone marrow (HBM) with no evidence of disease (NED; defined as blasts <5% on nadir bone marrow biopsy) may also benefit from G-CSF, but the currently available literature is lacking. In addition, venetoclax administration duration greatly affects the period of cytopenia. Guidance states that venetoclax should be given daily in a 28-day cycle for induction; however, recent data suggest that shorter induction courses (7-14 days) may provide a similar response with fewer adverse events.1,5,6
The current practice at our institution varies from provider to provider, but nadir bone marrow biopsies are typically performed on day 21 of HMA plus venetoclax induction therapy to confirm if there is HBM with NED, and then another bone marrow biopsy is conducted at ANC recovery to assess for CR. Historically, most providers at our institution preferred to keep patients admitted in the hospital while receiving HMA plus venetoclax therapy for induction and through ANC recovery, but practices continue to evolve with more patients being moved to the outpatient setting for treatment. For patients who are admitted to our institution for HMA plus venetoclax induction therapy, if HBM with NED is not achieved with cycle 1, they will often remain inpatient and proceed with cycle 2 of induction therapy with similar assessments for response.
The primary objective of this study is to evaluate the time to ANC recovery for patients with HBM with NED after induction therapy with HMA plus venetoclax who received G-CSF versus those who did not receive G-CSF. The secondary objectives are to evaluate the duration of induction therapy with HMA plus venetoclax, the safety of G-CSF use in patients with HBM with NED after induction therapy with venetoclax, and to determine the financial characteristics associated with induction therapy when comparing patients who received G-CSF versus patients who did not receive G-CSF.
Methods
This retrospective, single-center, cohort study evaluated the time to ANC recovery for patients with HBM with NED following induction with HMA plus venetoclax therapy who received G-CSF versus those who did not receive G-CSF. Patients were included if they were aged ≥18 years on day 1 of chemotherapy with a diagnosis of AML and received either azacitidine and venetoclax or decitabine and venetoclax for induction therapy between January 1, 2019, and May 31, 2024. In addition, patients had to have confirmed HBM with NED after induction therapy with one of the aforementioned regimens (after receiving up to 2 cycles of induction) to be included in the study. Patients were excluded from the study if they received any additional chemotherapy as a part of induction therapy.
At our institution, the standard is to prescribe posaconazole as first-line antifungal prophylaxis unless there are concerns for QTc prolongation, in which case we will use isavuconazole instead. To account for drug-drug interactions, our standard is to reduce the venetoclax dose by 75% when using posaconazole and by 50% when using isavuconazole. Patients who were to be screened were identified using Epic SlicerDicer. The data were collected through retrospective chart review using Research Electronic Data Capture (REDCap). REDCap is a secure, web-based software platform designed to support data capture for research studies. The study protocol was approved by the organization’s institutional review board.
The primary study end point was the time to ANC recovery (ANC >1 cell/L on 2 consecutive days or ANC >1.5 cells/L on 1 day) within 90 days from day 1 of chemotherapy. The secondary end points included the number of venetoclax doses administered, safety outcomes, and financial characteristics. The safety end points of interest included the rate of relapse within 6 months from day 1 of chemotherapy (defined as blasts ≥5% on postnadir bone marrow biopsy) and the rate of confirmed infection within 90 days from day 1 of chemotherapy (confirmed microbiologic data of bacterial, fungal, or viral infection). The financial characteristic end points of interest included the number of doses of G-CSF received for those in the G-CSF group and the length of hospital stay from day 1 of chemotherapy for both groups.
Statistical Analysis
Descriptive statistics for the demographic, clinical, and outcome characteristics were reported by the use of G-CSF (yes or no). The categorical variables were summarized using frequency and percentages, and the continuous variables were summarized with mean, standard deviation, median, quartile 1, quartile 3, and range. The number of missing values was reported for each characteristic.
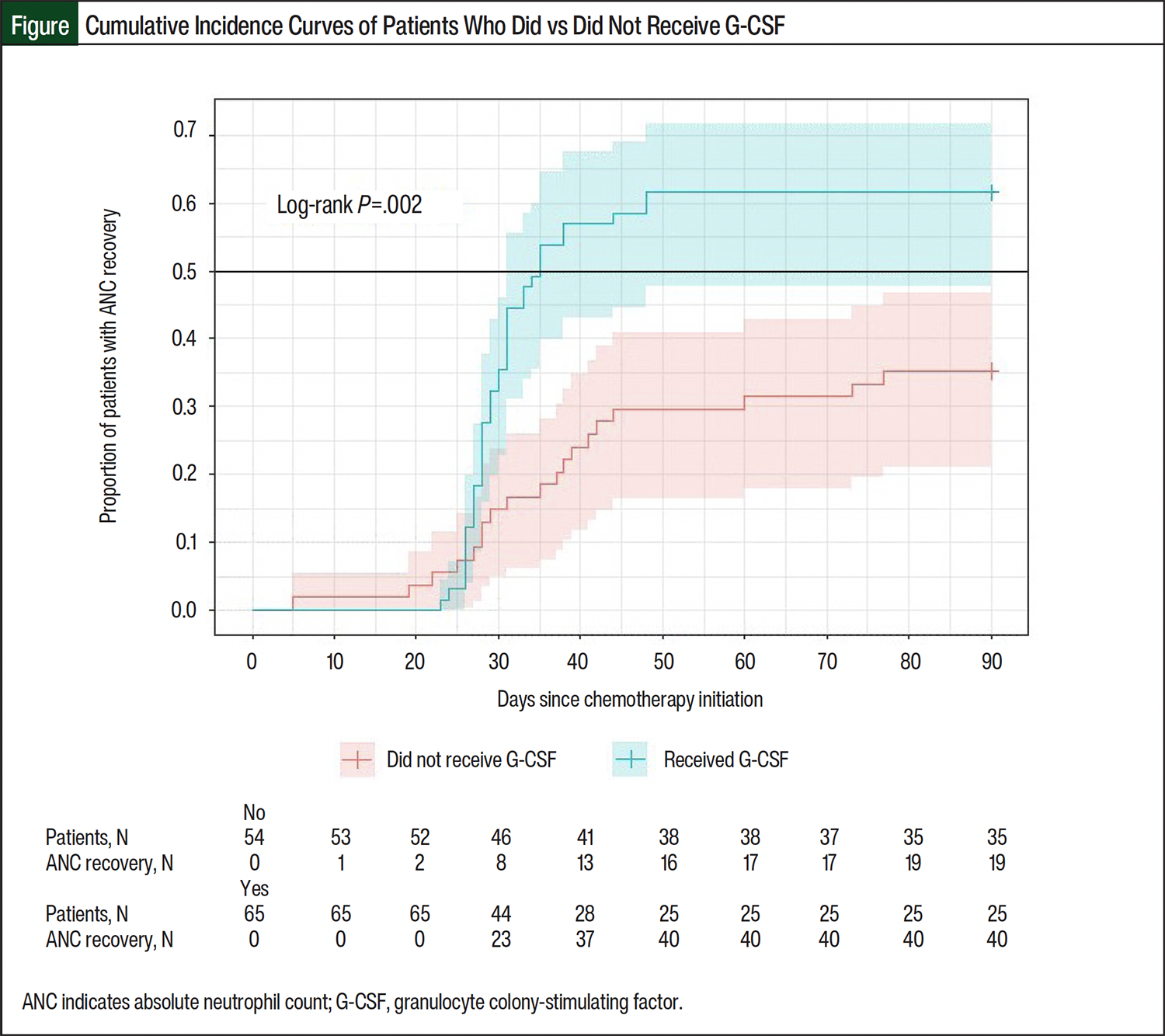
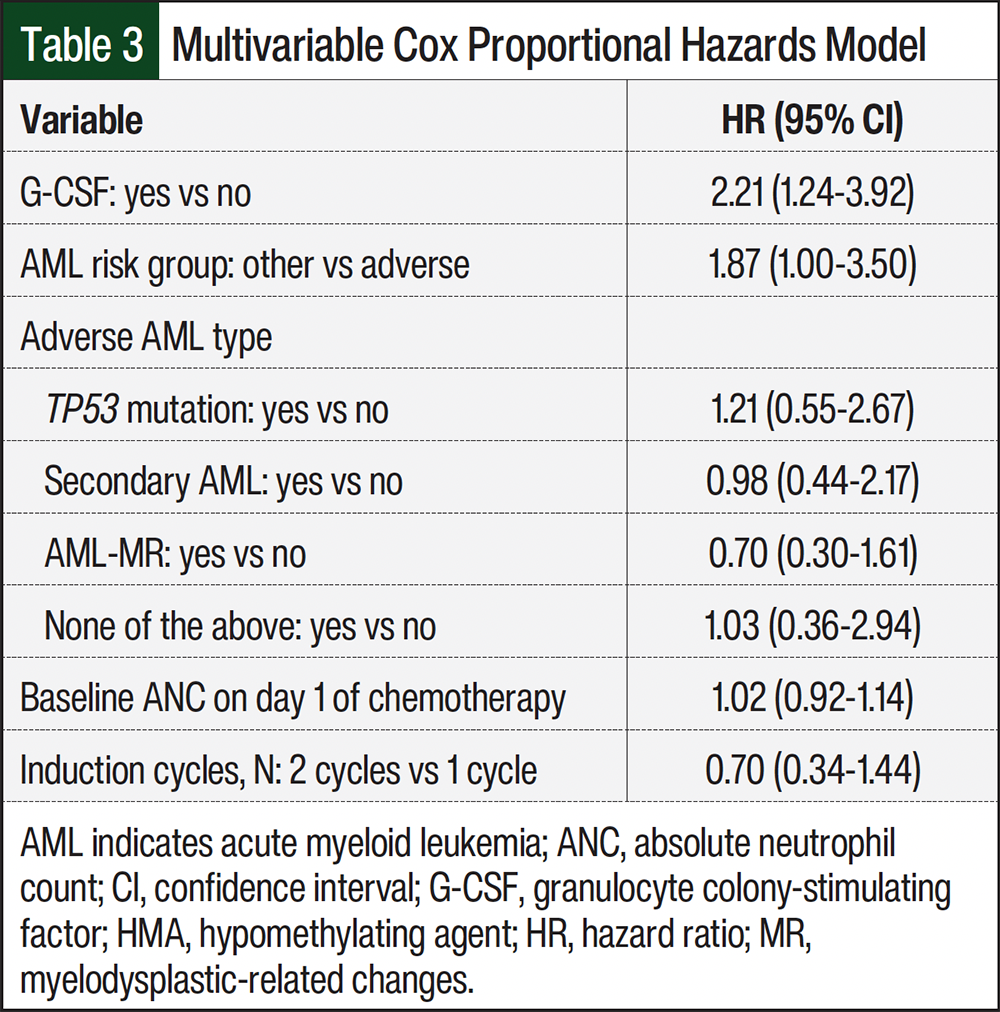
To assess the primary outcome, a Kaplan-Meier cumulative incidence curve by G-CSF group was plotted with the Greenwood formula for 95% confidence intervals (CIs) and was assessed using a log-rank test, with the level of significance set at 0.05. Patients were censored if they had not yet achieved ANC recovery and had not been discharged by the end of the study period (May 31, 2024) or at 90 days, whichever came first. In addition, a multivariable Cox proportional hazards model was fit to evaluate the primary outcome between patients with and without G-CSF while accounting for AML risk group, adverse AML type, baseline ANC, and number of induction cycles. Adverse AML risk was assessed using stratification criteria from the current AML guidelines.1 Cytogenetics and next-generation sequencing information were collected and assessed to determine if a patient fit into the adverse-risk category. The hazard ratio and 95% CI for G-CSF versus no G-CSF were reported.
The secondary safety and financial outcomes were analyzed descriptively by G-CSF, with differences in means or proportions and associated 95% CIs reported. All statistical analyses were performed in R version 4.4.0 (R Core Team; 2024).
Results
A total of 350 patients with AML who received HMA plus venetoclax therapy were screened for inclusion in the study (Appendix Figure S1). Of these patients, 119 met the inclusion criteria and 65 (54.6%) received G-CSF (Table 1). The overall median age was 74 years (interquartile range [IQR], 69-80) in both groups. The patients in both groups were predominantly White (73.9%) and non-Hispanic (95%). Most patients had adverse-risk AML (71.4%), including 34 (28.6%) with TP53 mutation, 25 (21%) with secondary AML, and 47 (39.5%) with AML with myelodysplastic-related changes.
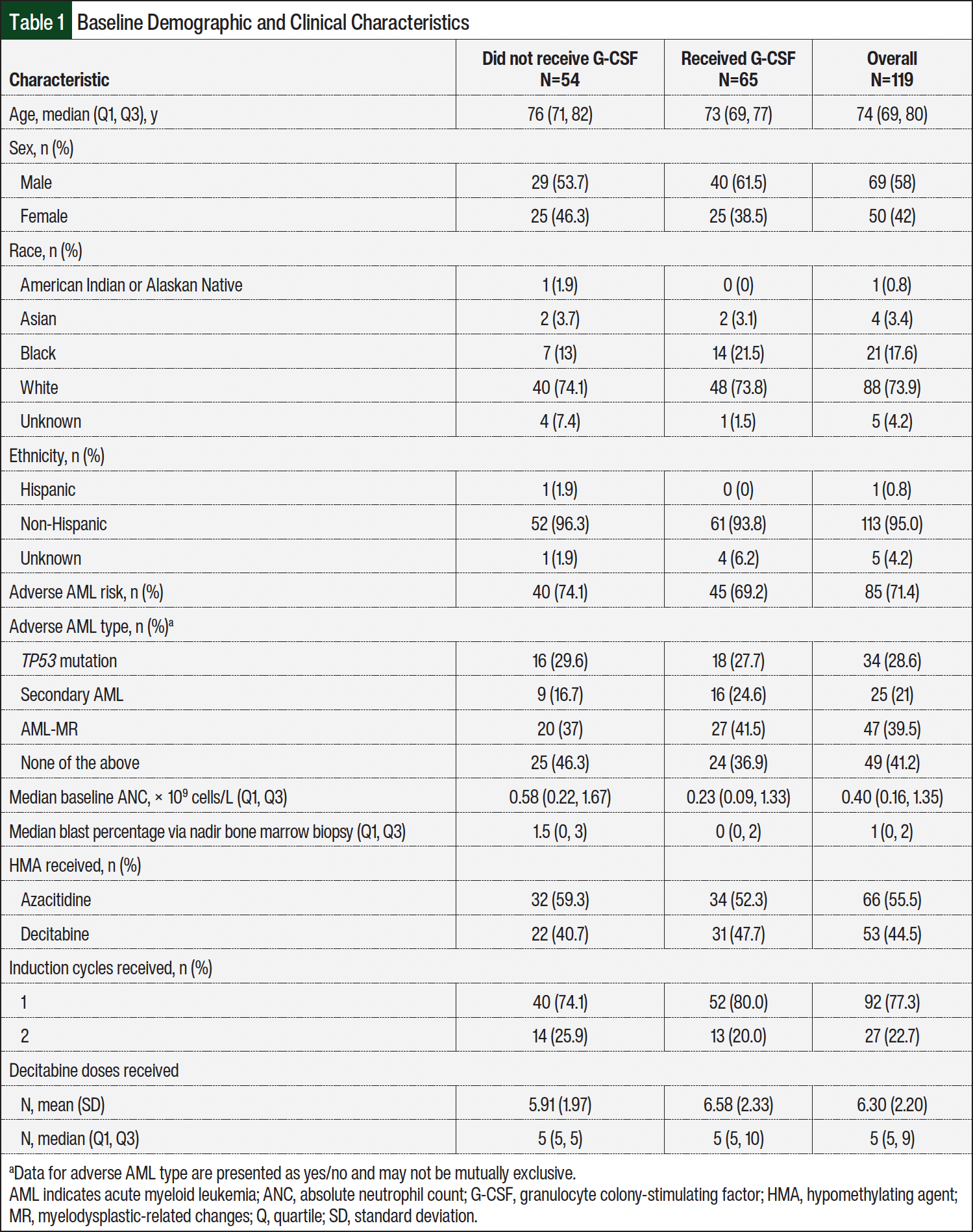
The median baseline ANC was higher in the patients who did not receive G-CSF at 0.58 cells/L (IQR, 0.22-1.67) compared with 0.23 cells/L (IQR, 0.09-1.33) in the patients who received G-CSF. The median blast percentage on the nadir bone marrow biopsy was also higher in patients who did not receive G-CSF versus those who did (1.5% vs 0%, respectively). Overall, slightly more patients received azacitidine (55.5%) than decitabine (44.5%) for induction therapy. Of those patients who received decitabine, the median number of doses received was 5 (IQR, 5-9). Most (77.3%) of the patients received only 1 cycle of induction before achieving HBM with NED on their nadir bone marrow biopsy.
The primary and secondary study outcomes are summarized in Table 2. Among the patients who reached ANC recovery, the median time to recovery was shorter in the patients who received G-CSF versus the patients who did not (29 days vs 37 days, respectively). The Kaplan-Meier cumulative incidence function of ANC recovery was plotted by G-CSF (Figure). Of the patients who received G-CSF, 61.5% had ANC recovery within 90 days from day 1 of chemotherapy, which was significantly higher than only 35.2% of patients who did not receive G-CSF (log-rank test; P=.002). The results of the Cox proportion hazards model are concordant with the conclusion from the cumulative incidence curves and associated log-rank test (Table 3). When controlling for factors associated with ANC recovery (AML risk group, adverse AML type, baseline ANC, and number of induction cycles), the ANC recovery at any given time point was 2.2 times higher for the patients who received G-CSF than for those who did not receive G-CSF (95% CI, 1.2-3.9).
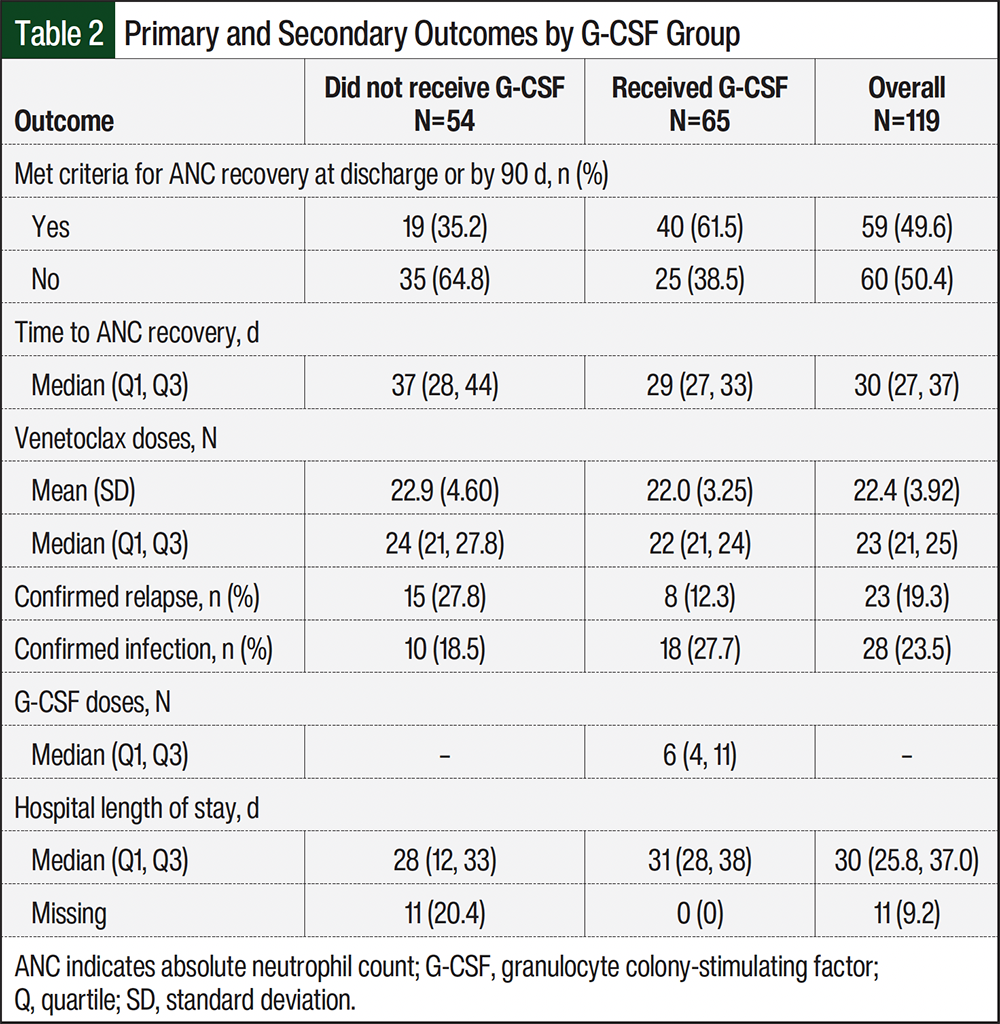
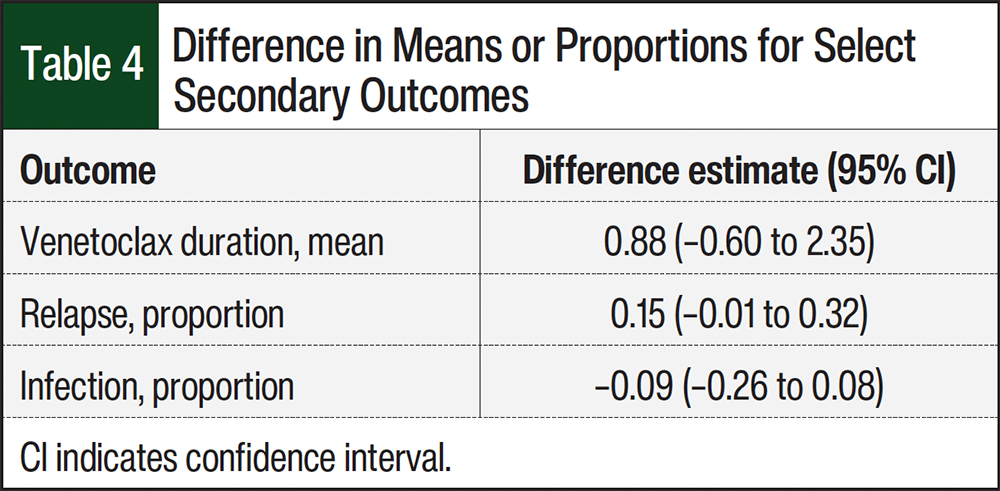
The descriptive statistics for the secondary outcomes are summarized in Table 2. The overall median number of venetoclax doses was 23 (IQR, 21-25). There were no significant differences between the 2 groups for the mean venetoclax treatment duration or the proportions of relapses and infections (Table 4). For the safety outcomes, the group that received G-CSF had a numerically lower rate of relapse (12.3% vs 27.8%) but a higher rate of infection (27.7% vs 18.5%) than the patients who did not receive G-CSF (Table 2). However, there were no significant differences in the proportions when the groups were compared.
For the financial characteristic end points, the 2 groups had similar hospital lengths of stay, with an overall median of 30 days (IQR, 25.8-37). Patients who received G-CSF were administered a median of 6 doses (IQR, 4-11). For financial characteristics, G-CSF was estimated to cost $300 per dose based on established institutional drug pricing, and a stay in the hospital was estimated to cost $3400 daily based on data from the Agency for Healthcare Research and Quality Healthcare Cost and Utilization Project from 2017.7 The median duration of G-CSF was 6 days (IQR, 4-11), making the total estimated price of G-CSF $1800 (IQR, $1200-$3300) per hospitalization for the patients who received it. The median hospital length of stay was 28 days (IQR, 12-33) for the patients who did not receive G-CSF and 31 days (IQR, 28-38) for the patients who received G-CSF, making the estimated bed costs $95,200 (IQR, $40,800-$112,200) and $105,400 (IQR, $95,200-$129,200), respectively. The total estimated price of hospitalization was calculated to be $95,200 (IQR, $40,800-$112,200) for the patients who did not receive G-CSF and $107,200 (IQR, $96,400-$132,500) for the patients who received G-CSF.
Discussion
The primary aim of this study was to evaluate the use of postnadir G-CSF in patients with AML who received induction therapy with HMA plus venetoclax. Although G-CSF is typically avoided in patients with AML because of its proliferative effects on myeloid cells, G-CSF may be an option without concern for disease progression in patients with AML who are in CR. Confirmatory evidence for efficacy and safety is needed for patients with HBM with NED.
This study shows that the time to ANC recovery was significantly shorter for patients who received G-CSF than for patients who did not receive G-CSF, even when accounting for potential confounders such as adverse AML risk, adverse AML type, and the number of induction cycles. There was a statistically significant increase in the proportion of patients who achieved early ANC recovery for the group that received G-CSF. There were no significant differences in the rate of relapse or incidence of infections between the 2 groups; however, there was a higher number of confirmed infections in the group that received G-CSF. It is unclear why infection rates were higher in this group; however, it is possible that, because of the retrospective nature of this study, providers were more inclined to start G-CSF treatment in patients with suspected infections.
These findings suggest that G-CSF is safe for use in patients who have HBM with NED, as indicated by no significant difference in relapse or infection rates and similar hospital length of stay. Because a formal cost analysis was not performed, direct conclusions cannot be drawn about the total financial impact of G-CSF, but there may be a higher total price per hospitalization for patients who receive G-CSF versus those who do not.
According to the findings from the VIALE-A trial, HMA plus venetoclax is the standard of care for newly diagnosed patients with AML who are ineligible for intensive chemotherapy.3,8 A recently published exploratory post hoc analysis of the VIALE-A trial evaluated outcomes of the use of G-CSF after blast clearance in patients who received HMA plus venetoclax.8 Approximately 50% of the patients in the VIALE-A trial received postremission G-CSF. The median time to neutrophil recovery from the first postremission grade 4 neutropenia was shorter for patients who received G-CSF (12 days) than for those who did not receive G-CSF (21 days), which is similar to our findings. The VIALE-A trial results showed that grade ≥3 infections occurred more often in patients who received G-CSF (65%) than in those who did not (49%), which correlates with the findings in this study and the idea that the retrospective nature of this study may have had an impact on the rate of infection between groups. Overall, the VIALE-A post hoc analysis showed no safety concerns and no negative impact on the duration of response or overall survival.8 Although this study did not evaluate the duration of response or overall survival explicitly, there were no differences in relapse rates. Other studies evaluating the use of G-CSF in AML induction showed similar results in terms of improving the time to count recovery without increasing the risk for relapse.9,10
One of the logistical challenges of using G-CSF during HMA plus venetoclax induction therapy is the 28-day duration of venetoclax. The VIALE-A protocol recommended 28 days of venetoclax therapy during the first cycle. Modifications, such as reducing the venetoclax duration, were allowed in subsequent cycles after achieving a CR to permit better integration of G-CSF during treatment with HMA plus venetoclax.3 At our institution, providers will often start G-CSF and stop venetoclax simultaneously if the nadir bone marrow biopsy shows HBM with NED during induction. This allows earlier support for count recovery and helps guide venetoclax duration for future cycles.
Limitations
This study had several limitations, primarily related to the retrospective and observational nature of this study. The study period began in January 2019 when treatment with HMA plus venetoclax was less familiar to providers at our institution. Because of the evolution of information over time, it is possible that there were changes in practice from the beginning to the end of this study period. These changes in practice may include variations in monitoring, duration of therapy, comfort with the use of G-CSF, and other supportive care measures used for these regimens, such as increased familiarity and comfort with the use of isavuconazole for antifungal prophylaxis rather than posaconazole. These changes were evident because the patients who received G-CSF tended to be treated later in the study period. With these gradual changes in practice over time, we likely now have more efficient follow-up for these patients in more recent years, which could account for the difference in hospital lengths of stay between groups.
There were also differential missing data for hospital length of stay between the groups, which could result from operational changes in time as well. Patients who received treatment outpatient or who were discharged before count recovery were included in this study, but the laboratory follow-up for these patients was inconsistent. This may have led to missing data and a possible impact on the results seen primarily in patients who did not receive G-CSF. Patients could also receive azacitidine or decitabine (including a 5- or 10-day treatment course), which could impact the time to count recovery. In addition, the study period began before the COVID-19 pandemic, continued through it, and then ended soon after the pandemic ended. It is likely that patients would have received the same HMA plus venetoclax therapy with or without G-CSF regardless of the pandemic, but because most of the patients who received G-CSF tended to receive treatment later in the study period, we cannot rule out the influence of the pandemic.
Last, we had limited financial information to draw conclusions on the financial impact of G-CSF use in this patient population. Some of the financial information used is from 2017, and the actual estimated costs may be higher than presented in this study. Further financial data are needed to draw more definitive conclusions.
Conclusion
In this single-center, retrospective study, the use of G-CSF significantly decreased the time to ANC recovery for postnadir patients with AML who received induction therapy with HMA plus venetoclax. Although there were no significant differences in relapse or infection outcomes observed between the G-CSF groups, further studies with larger sample sizes are needed to more definitively assess the comparability of safety outcomes. The total estimated cost of hospitalization was higher for patients who received G-CSF than for those who did not; however, further financial data are needed.
This study highlights an important opportunity for interdisciplinary discussion in the management of patients with AML with HBM with NED. Each patient must be thoroughly assessed by providers and pharmacists to determine the potential risks and benefits of the use of G-CSF. When used thoughtfully, G-CSF may be used to help support ANC recovery without compromising safety. Additional large-scale studies are needed to confirm the impact of G-CSF use on this patient population.
Disclosure Statement
Dr Clark, Dr Kennedy, Mr Reed, Ms Parish, Dr Lee, and Dr Huckabee have no disclosures to report.
References
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: acute myeloid leukemia. Version 3.2026. November 24, 2025. Accessed October 11, 2026. www.nccn.org/professionals/physician_gls/pdf/aml.pdf
- Jin S, Cojocari D, Purkal JJ, et al. 5-azacitidine induces NOXA to prime AML cells for venetoclax-mediated apoptosis. Clin Cancer Res. 2020;26:3371-3383. doi:10.1158/1078-0432.CCR-19-1900
- DiNardo CD, Jonas BA, Pullarkat V, et al. Azacitidine and venetoclax in previously untreated acute myeloid leukemia. N Engl J Med. 2020;383:617-629. doi:10.1056/NEJMoa2012971
- Link H. Current state and future opportunities in granulocyte colony-stimulating factor (G-CSF). Support Care Cancer. 2022;30:7067-7077. doi:10.1007/s00520-022-07103-5
- Cui J, Chen X, Li C, et al. Reduced duration and dosage of venetoclax is efficient in newly diagnosed patients with acute myeloid leukemia. Hematology. 2024;29:2293512. doi:10.1080/16078454.2023.2293512
- Bazinet A, Dinardo CD, Arani N, et al. A retrospective comparison of abbreviated course “7+7” vs standard hypomethylating agent plus venetoclax doublets in older/unfit patients with newly diagnosed acute myeloid leukemia. J Clin Oncol. 2024;42(suppl 16):Abstract 6507.
- Roemer M. Cancer-Related Hospitalizations for Adults, 2017. Agency for Healthcare Research and Quality. January 2021. Accessed May 12, 2025. https://hcup-us.ahrq.gov/reports/statbriefs/sb270-Cancer-Hospitalizations-Adults-2017.jsp
- DiNardo CD, Pratz KW, Panayiotidis P, et al. The impact of post-remission granulocyte colony-stimulating factor use in the phase 3 studies of venetoclax combination treatments in patients with newly diagnosed acute myeloid leukemia. Am J Hematol. 2025;100:185-188. doi:10.1002/ajh.27515
- Bouligny IM, Kantarjian HM, Yilmaz M, et al. Safety and efficacy of G-CSF with intensive chemotherapy in newly diagnosed acute myeloid leukemia: a subgroup analysis of the phase II trial of venetoclax in combination with cladribine, idarubicin, and cytarabine. Blood. 2024;144(suppl 1):446-448. doi:10.1182/blood-2024-203938
- Maeda T, Najima Y, Kamiyama Y, et al. Effectiveness and safety of primary prophylaxis with G-CSF after induction therapy for acute myeloid leukemia: a systematic review and meta-analysis of the clinical practice guidelines for the use of G-CSF 2022 from the Japan Society of Clinical Oncology. Int J Clin Oncol. 2024;29:535-544. doi:10.1007/s10147-023-02465-0