Connecting Science to Practice
There is a high risk for infusion-related reactions (IRRs)
with intravenous (IV) amivantamab. The prescribing information
for amivantamab recommends continuing
glucocorticoid premedication beyond the second dose if
an IRR occurs. In a quality improvement project aimed
to improve compliance with premedication recommendations,
a hard stop was added to a provider communication
within the treatment plan for IV amivantamab on
cycle 1 day 8. Providers were asked to review the medical
record and add glucocorticoid premedication if an IRR
occurred with a previous dose. This intervention numerically
improved premedication compliance among a small
sample of patients, suggesting that a simple modification
to the treatment plan can alter ordering patterns and
improve adherence to treatment recommendations.
The development of targeted therapies for lung adenocarcinoma has improved overall survival for patients with actionable mutations. EGFR mutations result in constitutive receptor activation, enhancing tumor growth and proliferation.1,2 EGFR mutations occur in approximately 20% of White patients and 50% of Asian patients with non–small cell lung cancer (NSCLC).1,3 Together the exon 19 deletion and the L858R point mutation in exon 21 comprise approximately 85% of EGFR mutations in NSCLC and are frequently targeted with EGFR tyrosine kinase inhibitors (TKIs), such as erlotinib and osimertinib.1 EGFR exon 20 insertion mutations, which comprise 4% to 10% of all EGFR mutations, are associated with a poor prognosis.4
Amivantamab is a bispecific antibody that targets activating and TKI-resistant EGFR mutations and MET receptor mutations and amplifications.5 Amivantamab was initially approved by the FDA in 2021 for locally advanced or metastatic EGFR exon 20 insertion–positive NSCLC after disease progression on platinum-based chemotherapy in accordance with the results of the CHRYSALIS trial.6,7 It received 3 additional FDA approvals for advanced or metastatic NSCLC in 2024 based on improved progression-free survival: as first-line treatment for EGFR exon 20 insertion–positive disease in combination with carboplatin and pemetrexed, and for patients with an EGFR exon 19 deletion or L858R mutation with lazertinib in the first-line setting and with carboplatin and pemetrexed after disease progression after receiving osimertinib.8-10 The recommended dose of intravenous (IV) amivantamab when administered without chemotherapy is 1050 mg for patients weighing <80 kg and 1400 mg for patients weighing ≥80 kg.6 Amivantamab is administered intravenously over a 28-day cycle as a split initial dose of 350 mg on cycle 1 day 1 and 700 mg (<80 kg) or 1050 mg (≥80 kg) on cycle 1 day 2, followed by a full dose administered weekly on days 8, 15, and 22 and biweekly beginning with cycle 2.
Infusion-related reactions (IRRs) have been reported with numerous monoclonal antibodies for the treatment of cancer.11 In contrast to immunoglobulin E–mediated anaphylactic reactions, IRRs are believed to be mediated by the release of cytokines from circulating leukocytes on binding of the monoclonal antibody to its target. The severity of IRRs is defined by the Common Terminology Criteria for Adverse Events.12 The clinical presentation of mild-to-moderate IRRs can include chills, fever, hypotension, tachycardia, dyspnea, rash, urticaria, erythema, and abdominal, muscle, or joint pain.6,11 These reactions are typically managed by temporarily withholding the drug, modifying the infusion rate, and/or administering supportive treatment with antihistamines, steroids, analgesics, and oxygen. Severe IRRs are less common, but may consist of severe hypotension and cardiac dysfunction. In severe cases, the infusion must be discontinued while appropriate pharmacotherapy and supportive care are administered.
IRRs were reported in 75 (66%) of the 114 patients in the safety population of the CHRYSALIS trial, representing the second most common adverse event (AE) after rash (86%).7 Most IRRs occurred on cycle 1 day 1 (93%) or cycle 1 day 2 (4%), with only 1 event reported after cycle 2. Grade ≥3 IRRs occurred in 3% of patients in CHRYSALIS. The prevalence of infusion reactions was consistent in later trials of amivantamab. IRRs were reported in 42% (grade ≥3, 1%) of patients who received amivantamab with carboplatin and pemetrexed in the PAPILLON trial and in 63% (grade ≥3, 6%) of patients who received amivantamab with lazertinib in the MARIPOSA trial.8,9 To reduce the risk for IRRs in the CHRYSALIS trial, the first dose of amivantamab was administered via a peripheral line at 25 mL/h during the first 2 hours and increased to 50 mL/h if tolerated.7 Premedication with an antihistamine (diphenhydramine) and antipyretic (acetaminophen) was required with all doses in addition to a glucocorticoid with cycle 1 days 1 and 2. Steroid premedication was not required with subsequent doses, but was recommended among patients who had an IRR. In the CHRYSALIS trial, 51% of patients received an optional steroid on cycle 1 day 8, and the rate of steroid premedication declined with further treatment.13 The prescribing information for amivantamab mirrors the CHRYSALIS protocol, requiring steroid administration before only the first 2 doses while suggesting continued utilization on cycle 1 day 8 and beyond after an IRR.6
Various tools exist to optimize treatment plans within the Epic electronic medical record (EMR). Beacon is the medical oncology module of Epic that facilitates the creation and implementation of treatment plans.14 A placeholder is a tool in Epic that can be included within an order set, treatment plan, or note template to indicate the need for user input or review. This creates a hard stop, prohibiting the user from signing the order or note without addressing or deleting the placeholder.
Data from our single, large academic cancer center showed that glucocorticoid premedication was not consistently continued beyond cycle 1 day 2 in patients who had an IRR after receiving an earlier dose of amivantamab, with 50% compliance over a 14-month period. Steroid premedication was built into the treatment plan for cycle 1 days 1 and 2, but required manual addition to all subsequent doses if an IRR occurred. In August 2024, we implemented a process improvement initiative aimed at increasing the number of patients who receive steroid premedication on cycle 1 day 8 after an IRR. The objective of this study was to compare the rate of steroid premedication compliance with the cycle-1 day-8 dose of amivantamab among patients who had an IRR after receiving a previous dose of amivantamab before and after adding the hard stop to the treatment plan.
Methods
This single-center, retrospective cohort study examined the effect of a process change on the ordering patterns of glucocorticoid premedication for amivantamab at The University of Texas MD Anderson Cancer Center, in Houston. The previous version of the amivantamab treatment plan included dexamethasone premedication on cycle 1 days 1 and 2, but it had to be added manually to all subsequent doses if an IRR occurred. In August 2024, the Beacon treatment plan for IV amivantamab within the Epic EMR was modified to add a placeholder hard stop on cycle 1 day 8 within a provider communication to alert the ordering provider to assess for previous IRRs and order dexamethasone premedication for cycle 1 day 8 and subsequent doses if appropriate. This prohibited providers from signing the cycle-1 day-8 order without addressing the notification. The placeholder could be removed after acknowledgment by the ordering provider, after which the cycle-1 day-8 order could be signed. Providers were educated not to prematurely delete the placeholder or sign orders for cycle 1 day 8 until after a patient receives the doses on cycle 1 days 1 and 2.
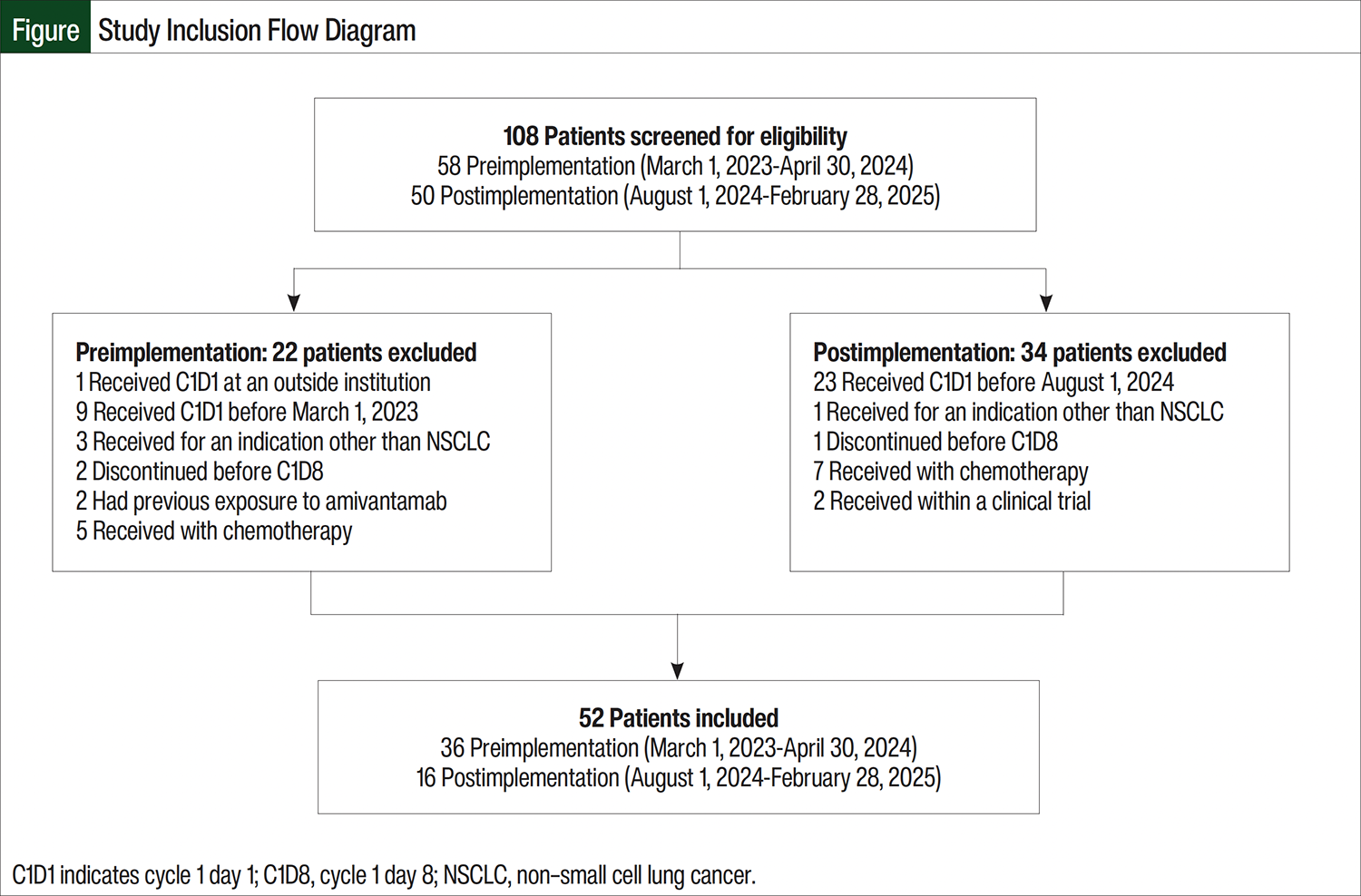
The study was approved by the institution’s Quality Improvement Assessment Board. The preimplementation cohort consisted of all patients who received amivantamab at our institution between March 1, 2023, and April 30, 2024. The treatment plan was updated on August 1, 2024, and the postimplementation cohort consisted of all patients who received amivantamab between August 1, 2024, and February 28, 2025. Patients were included if they received the first dose of amivantamab during the study period and received the cycle-1 day-1, day-2, and day-8 doses at the institution. Patients were excluded from the study if they received amivantamab for any indication other than NSCLC, as part of a clinical trial protocol, in combination with chemotherapy, or if they had any previous exposure to amivantamab in an earlier line of treatment.
The primary end point was to compare the rate of steroid premedication compliance on cycle 1 day 8 among patients who had an IRR after receiving a previous dose of amivantamab. The presence of an IRR was defined by the explicit documentation of an IRR in the medical record; the documentation of chills, fever, hypotension, tachycardia, dyspnea, rash, urticaria, erythema, or transient abdominal, muscle, or joint pain; or the administration of an antihistamine, H2 receptor antagonist, corticosteroid, or antipyretic during the same clinic encounter but after the initiation of the amivantamab infusion. A secondary end point was the rate of recurrent IRRs.
The data were collected retrospectively from the EMR of patients who received cycle-1 day-1 amivantamab before and after the implementation of the hard stop. These data included the patients’ demographic information, primary cancer diagnosis, amivantamab dose, route of administration, administration date and time, and the name, dose, and administration time of all additional medications administered on the day of the encounter. Administration time was recorded when the nurse charted each medication as administered.
Statistical Analysis
Statistical analysis was conducted using Minitab Statistical Software, version 21.4 (2023; Minitab, LLC; State College, PA). The primary and secondary end points and the rate of IRRs were analyzed using Fisher’s exact test with a significance level of 0.05.
Results
A total of 108 unique patients received amivantamab during the study period, and 52 patients met the criteria for inclusion. The preimplementation cohort consisted of 36 patients who received the first dose of amivantamab between March 1, 2023, and April 30, 2024, and the postimplementation cohort consisted of 16 patients who initiated amivantamab between August 1, 2024, and February 28, 2025. The most common reasons for exclusion were the receipt of cycle 1 day 1 before the study period and administration with chemotherapy (Figure).
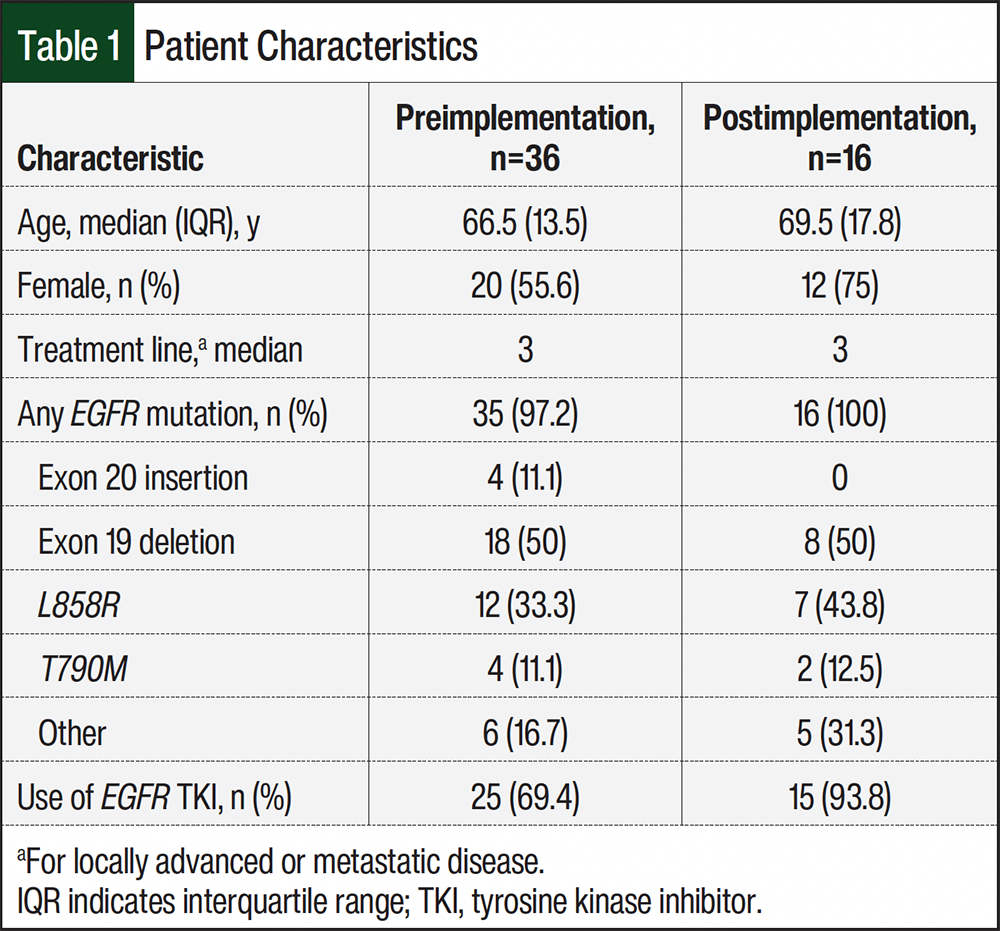
The patients’ baseline characteristics were similar between the 2 cohorts, with some variation attributable to the small sample size (Table 1). The patients received a median of 2 previous lines of systemic therapy for locally advanced or metastatic disease. With the exception of 1 patient who had an MET exon 14 skipping mutation, all patients had a documented EGFR mutation. Classical EGFR mutations were more common than the exon 20 insertion mutation. Concomitant TKI utilization was more frequent in the postimplementation group, which may reflect the publication of data supporting combination therapy for patients with classical EGFR mutations.9
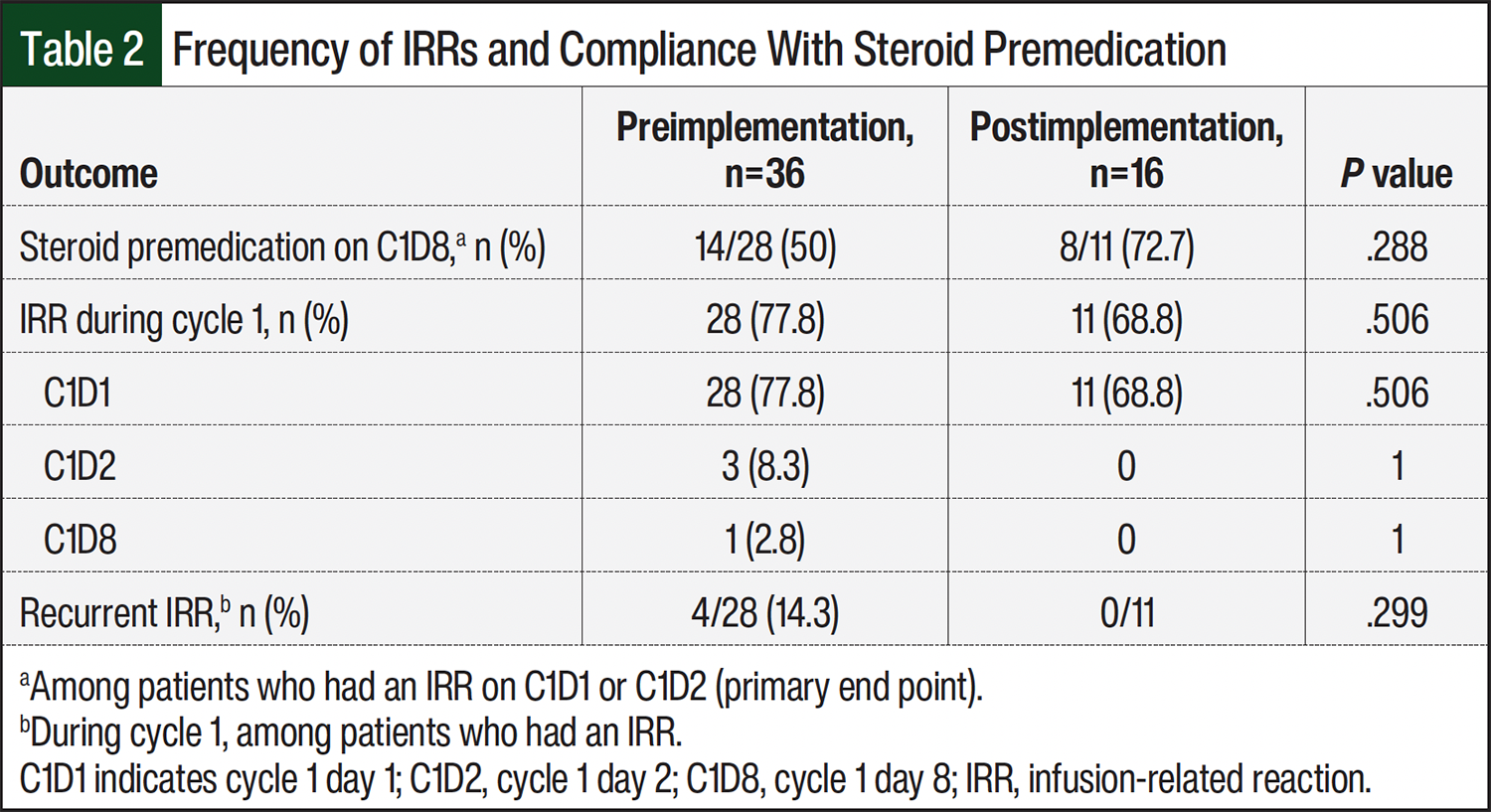
IRRs were observed in 28 (77.8%) of the 36 patients in the preimplementation cohort and in 11 (68.8%) of the 16 patients in the postimplementation cohort (Table 2). All patients with an IRR had it after receiving the first dose of amivantamab, and 4 (11.1%) patients in the preimplementation cohort had a recurrent IRR after receiving a subsequent dose of amivantamab. Steroid premedication was administered on cycle 1 day 8 to 14 (50%) of the 28 patients who had an IRR before the implementation of the alert and to 8 (72.7%) of the 11 patients who had an IRR after the implementation of the alert (P=.288). There was no significant difference between the preimplementation and the postimplementation cohorts in the rate of steroid premedication compliance on cycle 1 day 8.
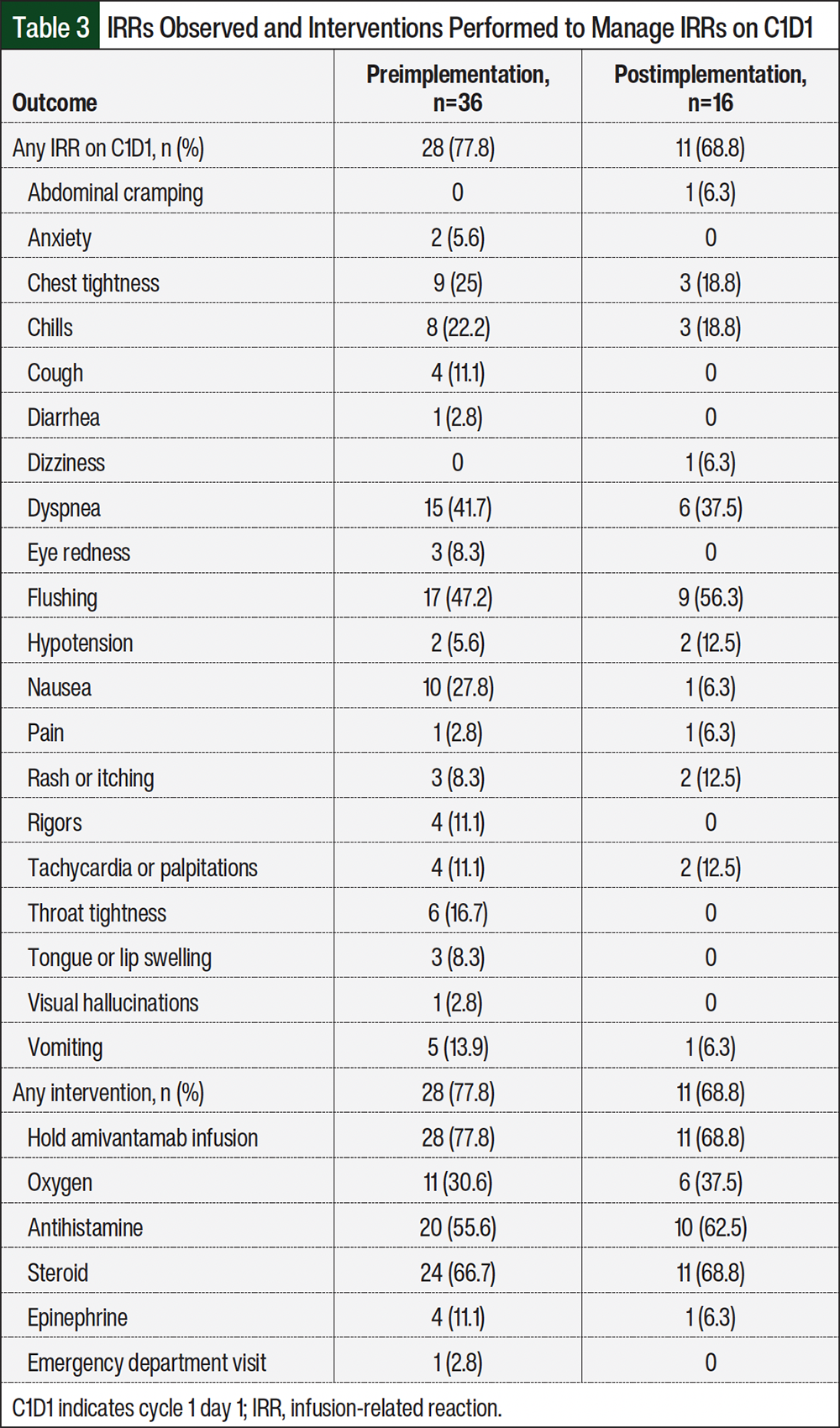
The frequency of specific IRR symptoms and interventions necessary to manage IRRs are shown in Table 3. The amivantamab infusion was stopped for all patients who had an IRR and was resumed at a slower rate on the resolution of symptoms. Most patients also received an additional dose of a steroid (hydrocortisone) and an antihistamine (diphenhydramine). The most frequently reported IRRs were flushing, dyspnea, chest tightness, chills, and nausea. Grade ≥3 IRRs were reported in 4 (11.1%) patients in the preimplementation cohort and 1 (6.3%) patient in the postimplementation cohort.
Discussion
The addition of a placeholder hard stop on cycle 1 day 8 did not result in a significant improvement in the rate of glucocorticoid premedication compliance among patients who had an IRR. However, this study included only 52 patients, and the relative sizes of the preimplementation and postimplementation cohorts were not balanced. The small sample size and short postimplementation follow-up likely impacted the results, potentially precluding statistical significance. Longer follow-up would not have substantially affected the results because there was a shift in prescribing patterns at our institution. However, among the first 16 patients who initiated amivantamab after the notification was introduced, premedication compliance among patients with IRRs improved by more than 20%. These preliminary results represent a clinically significant change. Further data collection is required to determine the full impact of this intervention.
To be included in this study, patients were required to receive each of the first 3 doses of amivantamab at our institution to allow providers to review the EMR for IRRs on cycle 1 day 8. Patients were excluded if they received amivantamab in combination with cytotoxic chemotherapy because of the prevalence of steroid premedication within many chemotherapy regimens including carboplatin with pemetrexed, with which amivantamab was studied.8 The same rationale was applied when excluding patients who received amivantamab within a clinical trial. Patients were excluded if they had previous exposure to amivantamab because of the substantially lower risk for IRRs after the first dose.7
In previous trials, IRRs were uncommon after cycle 1 day 1 of amivantamab, occurring in <4% of patients.7-9 Our data reported a higher frequency (7.7%) of IRRs with subsequent doses. All 4 of these reactions occurred among patients who had an IRR after the first dose of amivantamab. The higher frequency of late IRRs in our analysis could be attributed to its small sample size. This study was not designed to evaluate if continuing steroid premedication reduced the rate of recurrent IRRs. Of the 4 patients with recurrent IRRs, 3 received dexamethasone premedication on cycle 1 day 8, and the 1 patient with an IRR on cycle 1 day 8 received steroid premedication before that dose. In the CHRYSALIS trial, the use of steroid premedication declined over time after cycle 1 day 8.13 To align with the manufacturer’s recommendations, the diminishing risk for IRRs over time, and the goal of minimizing AEs from long-term steroid exposure, our amivantamab protocol allowed steroid premedication to be discontinued per the provider’s discretion after cycle 1 day 8.
Strategies to reduce the burden of IRRs with amivantamab are currently under investigation. Results from the SKIPPirr study demonstrated a reduction in IRRs with early steroid premedication before IV amivantamab.15 Oral dexamethasone 8 mg was administered twice daily for 2 days before cycle 1 day 1 and 1 hour before the first amivantamab infusion alongside the standard premedication regimen of dexamethasone 10 mg intravenously, an antihistamine, and an antipyretic. Of the 41 patients in the SKIPPirr trial, 10 (24%) had an IRR, which was substantially lower than historical data. Our institution implemented a similar strategy in October 2024, omitting the 8-mg oral dose of dexamethasone on cycle 1 day 1, but maintaining the 10-mg IV dose. Of the 5 patients who were prescribed oral dexamethasone for 2 days before the first dose of amivantamab, 2 (40%) had an IRR on cycle 1 day 1 compared with 37 (78.7%) of the 47 patients who did not. The implementation of this strategy will hopefully decrease the incidence of IRRs on cycle 1 day 1, but it did not impact the primary analysis of this study, which was limited to patients who had an IRR on cycle 1 day 1 of treatment. In addition, a subcutaneous formulation of amivantamab and hyaluronidase was compared with IV amivantamab, both with concomitant lazertinib, among patients with disease progression after receiving osimertinib and platinum-based chemotherapy in the PALOMA-3 trial.16 Patients randomized to subcutaneous amivantamab with lazertinib had fewer IRRs than those randomized to IV amivantamab with lazertinib (13% vs 66%, respectively), with similar preliminary efficacy outcomes. Subcutaneous amivantamab was FDA approved in December 2025 and poses an attractive alternative to the IV formulation.17
Limitations
Several limitations to this study exist. Placeholders can be deleted at any time, which may preclude their visibility to providers on cycle 1 day 8 of treatment. To address this, we educated our providers to refrain from prematurely deleting the placeholder and avoid signing orders for cycle 1 day 8 and beyond until after patients receive the first 2 doses of amivantamab. When assessing for IRRs with previous doses, providers relied on nursing reports from the infusion clinic. Nurses at our institution were educated to document amivantamab IRRs within the allergy section of the EMR. However, cases have been reported within our institution where amivantamab-related IRRs were not properly documented, causing steroid premedication on cycle 1 day 8 to be inappropriately omitted. With any process change, education and collaboration with all persons involved is important to ensure successful outcomes.
Conclusion
The addition of a placeholder hard stop that alerts the ordering provider to assess for IRRs before cycle 1 day 8 of amivantamab numerically improved steroid premedication compliance, but the difference was not statistically significant. Interventions aimed to reduce IRRs, including early steroid premedication and the development of the subcutaneous amivantamab formulation, appear promising. Treatment with amivantamab is expanding after the drug received 3 FDA approvals in 2024, including 2 for patients with the more common EGFR exon 19 deletion and L858R mutations. It is necessary to leverage tools within the EMR to ensure safe and proper treatment with amivantamab.
Author Disclosure Statement
Dr Wang is on the Advisory Board of Janssen and has received honoraria from MJH Life Sciences; Dr Lewis is currently employed at Bristol-Myers Squibb, but not at the time of the study; Dr Roth and Dr Rivera have no conflicts of interest to report.
References
- Harrison PT, Vyse S, Huang PH. Rare epidermal growth factor receptor (EGFR) mutations in non-small cell lung cancer. Semin Cancer Biol. 2020;61:167-179. doi:10.1016/j.semcancer.2019.09.015
- Kris MG, Johnson BE, Berry LD, et al. Using multiplexed assays of oncogenic drivers in lung cancers to select targeted drugs. JAMA. 2014;311:1998-2006. doi:10.1001/jama.2014.3741
- Shi Y, Au JSK, Thongprasert S, et al. A prospective, molecular epidemiology study of EGFR mutations in Asian patients with advanced non-small-cell lung cancer of adenocarcinoma histology (PIONEER). J Thorac Oncol. 2014;9:154-162. doi:10.1097/jto.0000000000000033
- Yasuda H, Park E, Yun CH, et al. Structural, biochemical, and clinical characterization of epidermal growth factor receptor (EGFR) exon 20 insertion mutations in lung cancer. Sci Transl Med. 2013;5:216ra177. Erratum in: Sci Transl Med. 2014;6:225er1. doi:10.1126/scitranslmed.3007205
- Yun J, Lee SH, Kim SY, et al. Antitumor activity of amivantamab (JNJ-61186372), an EGFR-MET bispecific antibody, in diverse models of EGFR exon 20 insertion-driven NSCLC. Cancer Discov. 2020;10:1194-1209. doi:10.1158/2159-8290.CD-20-0116
- Rybrevant (amivantamab-vmjw) injection, for intravenous use [prescribing information]. Janssen Biotech, Inc; November 2025. Accessed April 10, 2026. www.accessdata.fda.gov/drugsatfda_docs/label/2025/761210s011lbl.pdf
- Park K, Haura EB, Leighl NB, et al. Amivantamab in EGFR exon 20 insertion-mutated non-small-cell lung cancer progressing on platinum chemotherapy: initial results from the CHRYSALIS phase I study. J Clin Oncol. 2021;39:3391-3402. doi:10.1200/JCO.21.00662
- Zhou C, Tang KJ, Cho BC, et al. Amivantamab plus chemotherapy in NSCLC with EGFR exon 20 insertions. N Engl J Med. 2023;389:2039-2051. doi:10.1056/NEJMoa2306441
- Cho BC, Lu S, Felip E, et al. Amivantamab plus lazertinib in previously untreated EGFR-mutated advanced NSCLC. N Engl J Med. 2024;391:1486-1498. doi:10.1056/NEJMoa2403614
- Passaro A, Wang J, Wang Y, et al. Amivantamab plus chemotherapy with and without lazertinib in EGFR-mutant advanced NSCLC after disease progression on osimertinib: primary results from the phase III MARIPOSA-2 study. Ann Oncol. 2024;35:77-90. doi:10.1016/j.annonc.2023.10.117
- Rombouts MD, Swart EL, van den Eertwegh AJM, Crul M. Systematic review on infusion reactions to and infusion rate of monoclonal antibodies used in cancer treatment. Anticancer Res. 2020;40:1201-1218. doi:10.21873/anticanres.14062
- US Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. November 27, 2017. Accessed August 1, 2024. https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf
- Park K, Sabari JK, Haura EB, et al. Management of infusion-related reactions (IRRs) in patients receiving amivantamab in the CHRYSALIS study. Lung Cancer. 2023;178:166-171. doi:10.1016/j.lungcan.2023.02.008
- Specialties. Epic Systems Corporation. Accessed March 14, 2025. www.epic.com/software/specialty-care/
- Spira AI, Paz-Ares L, Han JY, et al. Preventing infusion-related reactions with intravenous amivantamab-results from SKIPPirr, a phase 2 study: a brief report. J Thorac Oncol. 2025;20:809-816. doi:10.1016/j.jtho.2025.01.018
- Leighl NB, Akamatsu H, Lim SM, et al. Subcutaneous versus intravenous amivantamab, both in combination with lazertinib, in refractory epidermal growth factor receptor-mutated non-small cell lung cancer: primary results from the phase III PALOMA-3 study. J Clin Oncol. 2024;42:3593-3605. doi:10.1200/JCO.24.01001
- Rybrevant Faspro (amivantamab and hyaluronidase-lpuj) injection, for subcutaneous use [prescribing information]. Janssen Biotech, Inc; February 2026. Accessed April 13, 2026. www.accessdata.fda.gov/drugsatfda_docs/label/2026/761484Orig1s000correctedlbl.pdf