Connecting Science to Practice
Graft-versus-host disease (GVHD), a common adverse event
of allogeneic hematopoietic stem-cell transplantation
(HSCT), arises from donor T-lymphocyte–mediated immune
responses targeting recipient tissue. Tacrolimus is
widely used for GVHD prophylaxis because of its ability to
suppress T-cell activation. Although continuous intravenous
(CIV) tacrolimus has been the standard, twice-daily bolus
administration has emerged as an alternative, addressing
limitations like line accessibility and prolonged infusion
times. Overall, twice-daily bolus tacrolimus offers a practical
alternative to CIV, maintaining efficacy and safety with
proper monitoring in HSCT recipients.
Graft-versus-host disease (GVHD) is a common complication of allogeneic hematopoietic stem-cell transplantation (HSCT) that is associated with morbidity and nonrelapse mortality.1,2 GVHD results from interactions between donor immune mediators and the HSCT recipient’s tissue. GVHD can be classified as either acute GVHD (aGVHD) or chronic (cGVHD) based on the timing of presentation and the clinical symptoms.1 In general, the onset of aGVHD occurs earlier after HSCT than cGVHD and predominantly affects the skin, gastrointestinal (GI) tract, and liver.3 Donor T-lymphocytes stimulate proinflammatory cytokine release, resulting in tissue injury that can impact single or multiple organs and present as a maculopapular rash, diarrhea, nausea/vomiting, and/or jaundice.3 Immunosuppressive regimens that target donor lymphocytes prevent GVHD.3 The National Comprehensive Cancer Network cites that up to 50% of allogeneic HSCT recipients will develop aGVHD, despite receiving prophylactic immunosuppressants.1
A retrospective analysis showed that the cumulative incidence of aGVHD requiring treatment was 40.9%, of which 35.2% of the cases were classic aGVHD and 5.7% were delayed aGVHD.4 Calcineurin inhibitors, such as tacrolimus, are frequently used as the backbone immunosuppressant for GVHD prophylaxis. Calcineurin inhibitors impair T-cell–mediated cytotoxicity by binding to the 12-kDa FK506-binding protein and inhibiting calcineurin phosphatase.5 This results in a reduction of T-cell lymphocyte proliferation, decreasing the risk for GVHD.5 One of the first phase 3, open-label, multicenter studies that compared tacrolimus plus methotrexate with cyclosporine plus methotrexate after a human leukocyte antigen–identical sibling marrow HSCT determined that the patients who received tacrolimus had a lower incidence of grade 2 to 4 aGVHD (31.9% vs 44.4%, respectively; P=.01).6 Another phase 3, open-label, multicenter study also showed a reduction in the rates of grade 2 to 4 aGVHD in patients who had an unrelated donor HSCT when comparing tacrolimus with cyclosporine (56% vs 74%, respectively; P=.0002).7
Tacrolimus is available in oral and intravenous (IV) formulations. Institutions may select IV or oral administration based on patient- and protocol-specific factors. Depending on institutional formularies for tacrolimus, there is an option of sublingual administration via immediate-release capsules that can be opened and dissolved under the patient’s tongue. IV routes may be necessary depending on the patient’s needs (eg, an inability to swallow, absorption concerns). The prescribing information includes recommendations for administering tacrolimus as a continuous IV (CIV) infusion of 0.03 mg/kg daily (based on lean body weight) for GVHD prophylaxis.5 CIV infusion occupies a catheter lumen for a full 24 hours, resulting in decreased access for other medications and blood products. It is also important to note that, after dilution, tacrolimus is stable for 24 hours in normal saline or dextrose 5% in water according to the prescribing information.
Because of these potential limitations, some institutions have implemented dosing IV tacrolimus as a twice-daily bolus. Evidence for twice-daily bolus tacrolimus administration in adults for GVHD prophylaxis is limited to retrospective studies with small sample sizes.8 Hashmi and colleagues evaluated 66 adult HSCT recipients who received tacrolimus 0.02 mg/kg twice daily administered over 4 hours with target trough levels between 5 and 15 ng/mL. Most of the population received hematopoietic stem cells from a matched donor (49% matched, related and 44% matched, unrelated), whereas 7% had a mismatched, unrelated donor.8 The incidence of grade 2 to 4 aGVHD at day 100 was 37%, with 15% of patients having grade 3 or 4 aGVHD.8
These results were comparable with the Center for International Blood and Marrow Transplant Research’s (CIBMTR) historical rates of aGVHD (39% for matched related donor; 59% for unrelated donor).9 The incidence of acute kidney injury was 42% compared with the historical controls using tacrolimus- and methotrexate-based regimens that had a serum creatinine doubling in 63% of patients.8,10 Hypertension (new onset or requiring increase in home medication dose) was observed in 18% of patients, and neurotoxicity symptoms occurred in some patients, including headaches (15%), tremors (9%), and seizures (3%).8 The average tacrolimus blood concentration was 10.62 ng/mL for all patients who had at least 4 recorded measurements.8 The researchers concluded that tacrolimus twice daily does not increase the incidence of common adverse events (AEs) and has similar rates of aGVHD when compared with historical CIV data.8
In another retrospective, single-arm study conducted by Bacopoulos and colleagues, 104 adult HSCT recipients received twice-daily bolus tacrolimus administered over 2 hours.11 The 43 patients who received IV tacrolimus for the prevention of GVHD showed similar results to those of Hashmi and colleagues and to the CIBMTR: 34.9% of patients had grade 2 to 4 aGVHD and 18.6% had grade 3 to 4 aGVHD within 180 days of HSCT.11 The incidence rate of hypertension was 21%.11 Based on these collective results, the purpose of the current study was to compare the clinical impact of converting from CIV tacrolimus to twice-daily bolus tacrolimus in adults who underwent allogeneic HSCT.
Methods
This single-center, retrospective cohort review evaluated allogeneic HSCT recipients who had an order for IV tacrolimus and were identified using a clinical surveillance tool between September 2019 and September 2022. Patients at TriStar Centennial Medical Center receive IV tacrolimus if they cannot tolerate oral tacrolimus (eg, they have difficulty swallowing, absorption issues). In April 2021, IV tacrolimus administration was transitioned from CIV to twice-daily bolus dosing.
Patients were included in the study if they were aged ≥18 years and received IV tacrolimus for GVHD prophylaxis. Patients were excluded if they received IV tacrolimus for GVHD treatment. The patients were divided into 2 cohorts for tacrolimus administration, twice-daily bolus or CIV dosing. From September 2019 to March 2021, the patients received CIV tacrolimus, and from April 2021 to September 2022, the patients received twice-daily bolus tacrolimus. This study was approved by the center’s institutional review board.
The primary objective of the study was to determine the incidence of aGVHD by provider assessment at 100 days after HSCT (day 100). The secondary objectives were the percentage of therapeutic troughs, number of dose modifications, incidence of AEs (nephrotoxicity and hypertension requiring pharmacologic intervention), grading and incidence of aGVHD and cGVHD, disease relapse, and mortality. The extent of skin rash, total bilirubin level, and volume of diarrhea were assessed to stage and grade aGVHD using the Mount Sinai Acute GVHD International Consortium criteria.12 The National Institutes of Health’s consensus criteria for organ scoring was used by providers for the cGVHD diagnosis.13 The incidence of cGVHD was assessed from day 100 until the end of follow-up. Nephrotoxicity was defined using the Common Terminology Criteria for Adverse Events version 4.0 for acute kidney injury.14 Hypertension was defined as a requirement for a new antihypertensive agent or an increase in the dose of an existing antihypertensive agent after the initiation of IV tacrolimus. Therapeutic tacrolimus troughs were defined as a level between 5 and 15 ng/mL once at steady state. Falsely elevated levels of therapeutic tacrolimus (eg, laboratory tests drawn from contaminated lumen) were excluded from the study.
The data were collected retrospectively from the electronic medical record. The baseline demographics included HSCT indication, donor type, graft source, conditioning chemotherapy regimen, immunosuppressant regimen, and azole antifungal received. The tacrolimus dosing characteristics consisted of the types of administration (CIV or twice daily), duration of IV tacrolimus, number of dose modifications, and therapeutic drug-monitoring levels. The aGVHD outcomes included the time of onset, grade, organ involvement, and treatment regimen. Other outcomes included the cGVHD diagnosis, grade of nephrotoxicity, incidence of hypertension requiring pharmacologic intervention, relapse, readmission, and mortality.
Statistical Analysis
Continuous variables were described using the median and range, whereas categorical values were described using frequency and percentages. The data were reported as event incidence per total number of possible occurrences from the 2 cohorts. From these values, Fisher’s exact, chi-square, and Mann-Whitney U tests were performed; an alpha significance level of 0.05 was used for all tests.
Results
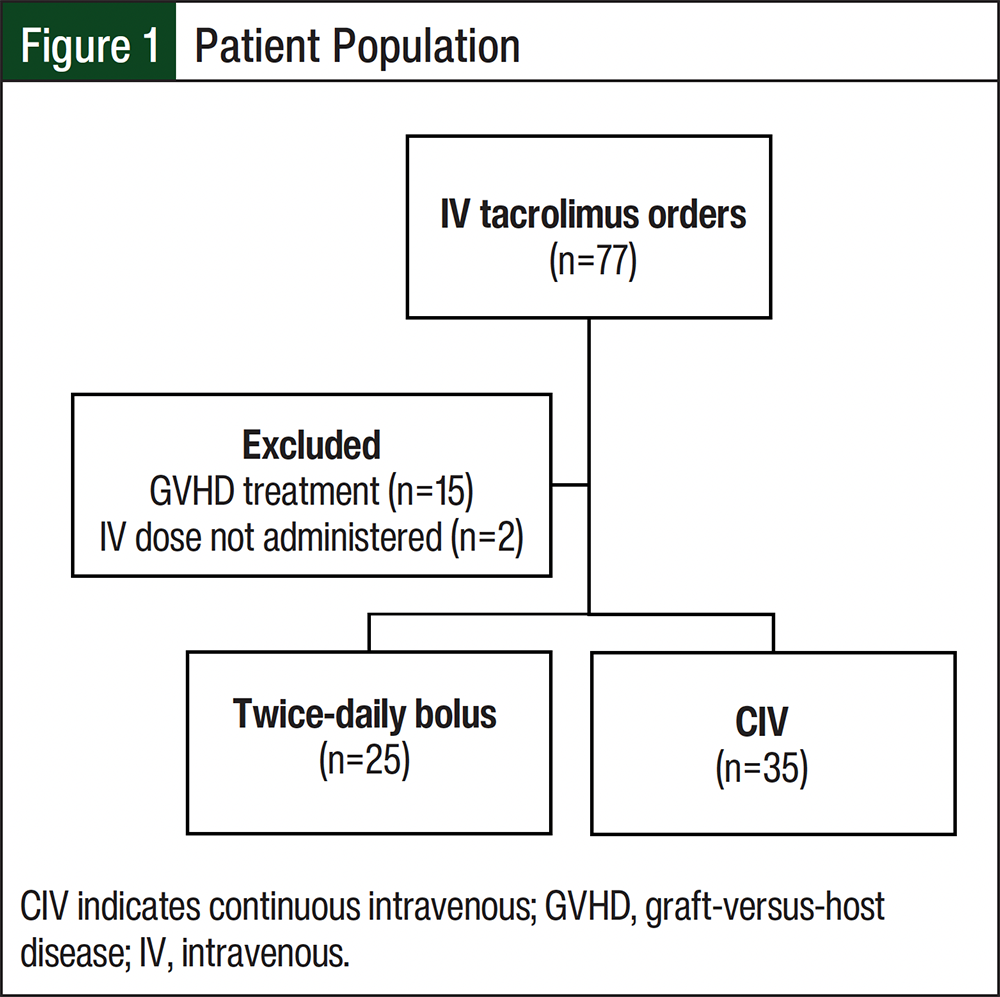
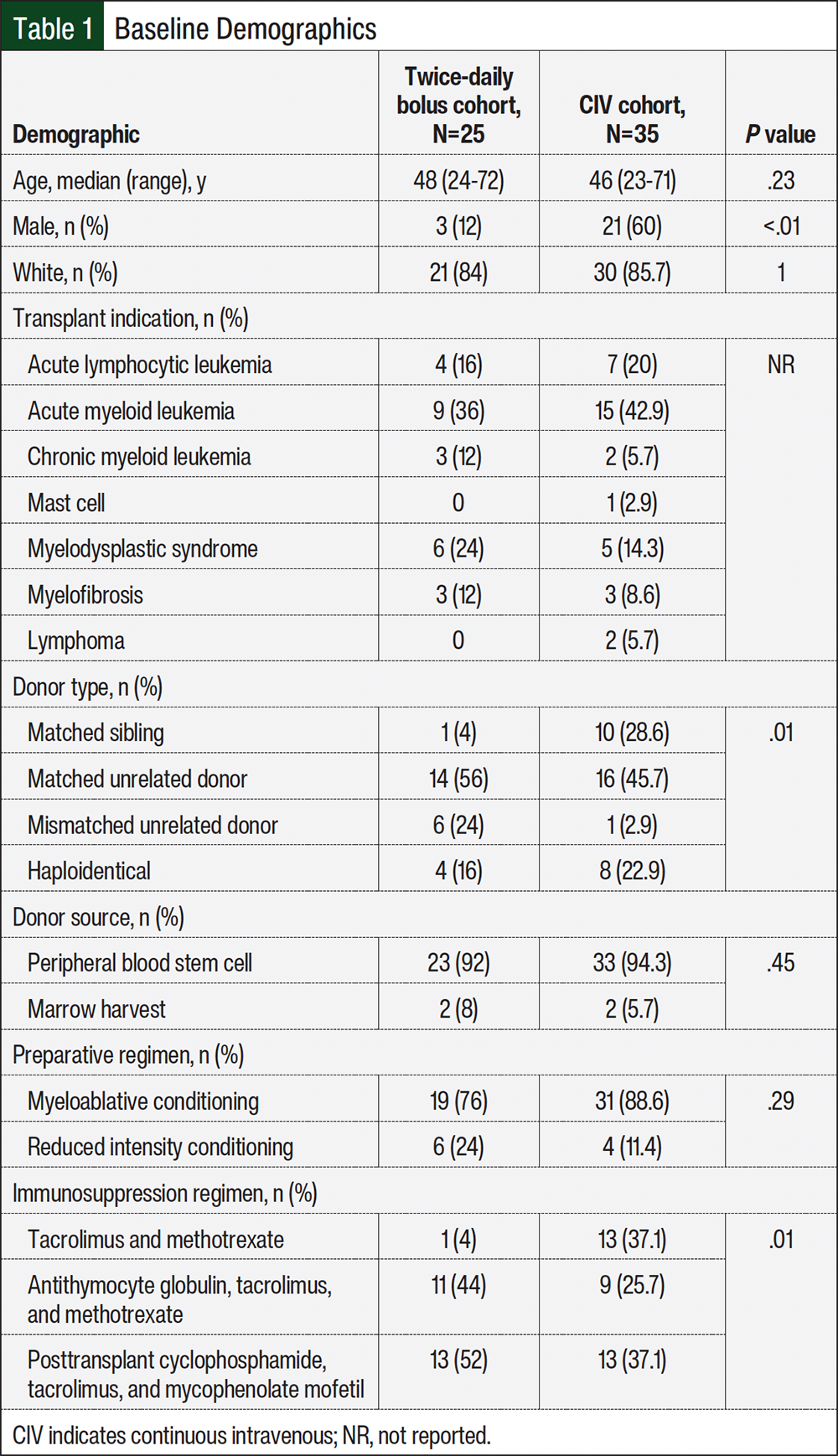
A total of 77 allogeneic HSCT recipients were identified as having an order for IV tacrolimus during the study time frame. In all, 15 patients were excluded from the study because tacrolimus had been used for the treatment of GVHD, and 2 patients were excluded because they did not receive a dose of IV tacrolimus (Figure 1). A total of 25 patients were included in the twice-daily bolus cohort and 35 were included in the CIV cohort (Table 1). The median age was similar between the twice-daily bolus and CIV cohorts (48 years vs 46 years, respectively; P=.23). Most patients in both cohorts were White, had a peripheral blood graft source, and received a myeloablative conditioning regimen. Acute myeloid leukemia was the most common indication for receiving allogeneic HSCT. Fewer patients in the twice-daily bolus cohort had a matched sibling donor compared with those in the CIV cohort (4% vs 28.6%, respectively). There were more matched unrelated donors (56% vs 45.7%, respectively) and mismatched unrelated donors (24% vs 2.9%, respectively) in the twice-daily bolus cohort versus the CIV cohort (P=.01). Immunosuppressant regimens for GVHD prophylaxis also varied between the 2 cohorts. More patients in the twice-daily bolus cohort received a combination of posttransplant cyclophosphamide, tacrolimus, and mycophenolate mofetil than those in the CIV cohort (52% vs 37.1%, respectively; P=.01).
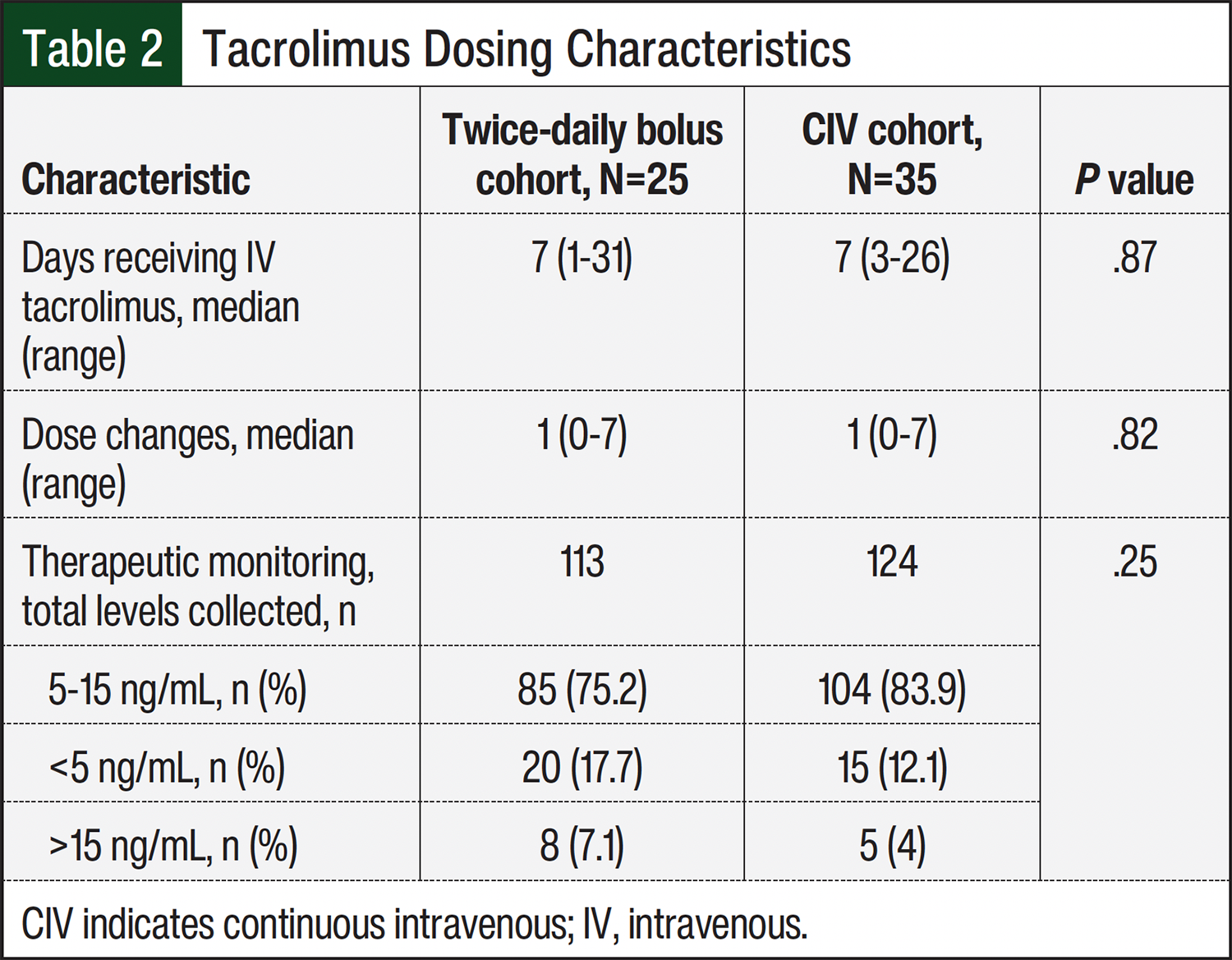
There was a total of 236 tacrolimus levels for the 60 patients in the study (Table 2). There was no difference in the percentage of therapeutic levels between the twice-daily bolus and CIV cohort (75.2% vs 83.9%, respectively; P=.25). The median duration of IV tacrolimus was 7 days for both cohorts (range, 1-31 days with twice-daily bolus vs 3-26 days with CIV; P=.87). In addition, the median number of dose modifications was 1 for both patient cohorts.
The incidence of aGVHD at day 100 in the twice-daily bolus cohort was 52% compared with 51.4% in the CIV cohort (P=1; Table 3). There was also no difference in the median time to onset, maximum overall grade, grade 2 to 4, or multiple sites of aGVHD. The median time to the onset of aGVHD was 33 days for the twice-daily bolus cohort versus 40 days for the CIV cohort (range, 17-98 days for twice-daily bolus vs 21-88 days for CIV; P=.59). Of the 25 patients who received a twice-daily bolus of tacrolimus, 11 (44%) had grade 2 to 4 aGVHD (P=.42). Of the 25 patients, 4 (16%) had grade 3 aGVHD, and none of the patients had grade 4 aGVHD (P=.38). Of the 35 patients in the CIV cohort, 11 (31.4%) had grade 2 to 4 aGVHD; 2 (5.7%) of the 35 patients had grade 3 aGVHD and 1 (2.9%) had grade 4 aGVHD.
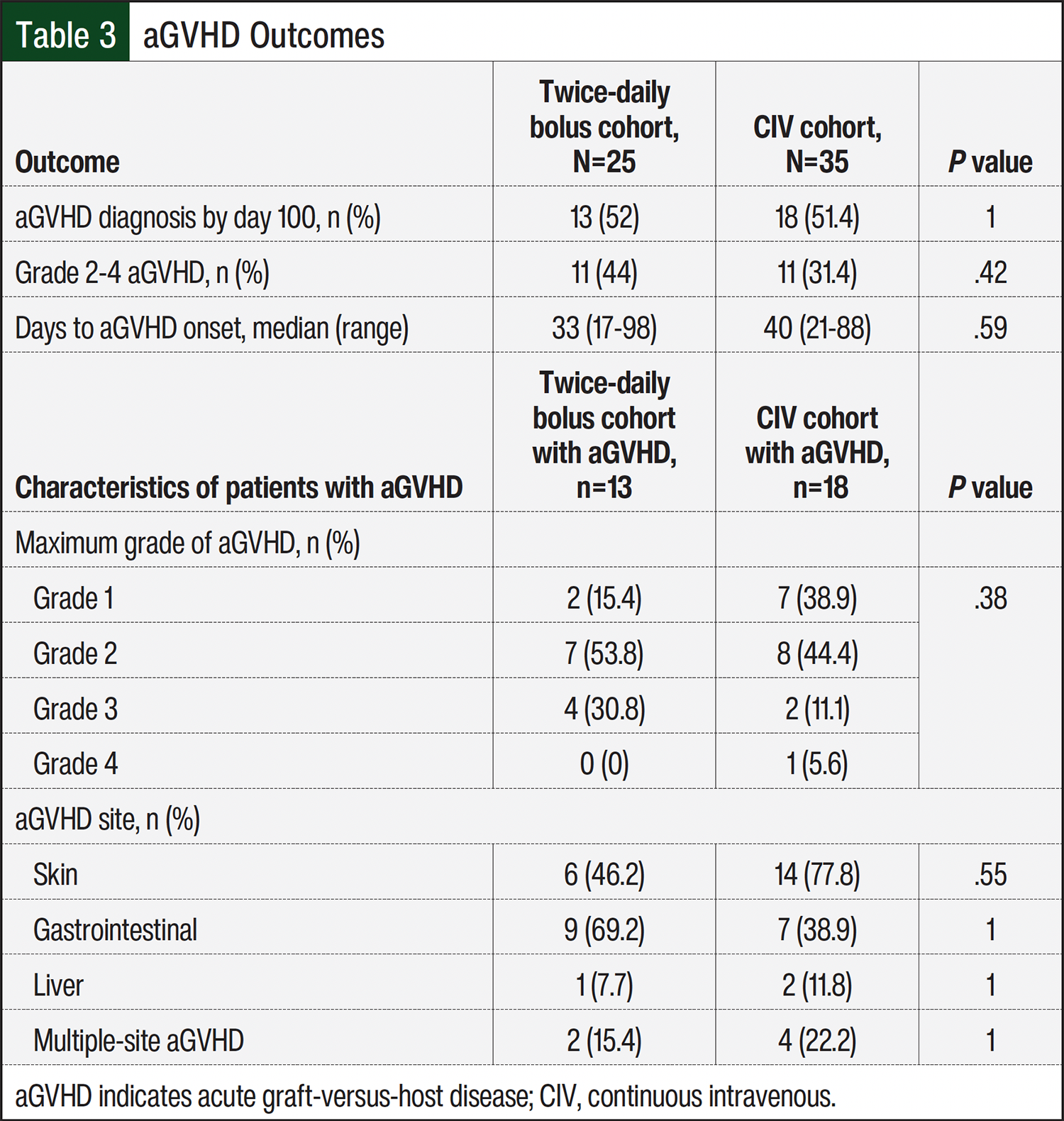
Overall, the organ systems affected by aGVHD (ie, the skin, GI system, liver) were similar between the cohorts (P=.27). Although not significantly different, there was a higher number of patients with GI tract site–related aGVHD in the twice-daily cohort (P=1) and more skin site–related aGVHD in the CIV cohort (P=.55). A total of 2 (15.4%) patients in the twice-daily bolus cohort and 4 (22.2%) patients in the CIV group had at least 2 sites of aGVHD. Of the 13 patients in the twice-daily bolus cohort who had aGVHD, 6 (46.2%) had aGVHD involving the skin, 9 (69.2%) had GI tract involvement, and 1 (7.7%) had liver involvement. Of the 18 patients in the CIV cohort who had aGVHD, 14 (77.8%) had skin involvement, 7 (38.9%) had GI tract involvement, and 2 (11.8%) had liver aGVHD. All patients received corticosteroids for the treatment of aGVHD; 4 patients in the twice-daily bolus cohort and 3 patients in the CIV cohort also received ruxolitinib, a JAK1 and JAK2 inhibitor. Two patients from each of the cohorts were readmitted by day 100 for the management of aGVHD (P=1).
The median duration of follow-up from the HSCT date until data collection was 2.5 years for the CIV cohort and 1 year for the twice-daily bolus cohort. A total of 12 (48%) patients in the twice-daily bolus cohort had cGVHD (Table 4), with 7 (58.3%) of these patients having a previous diagnosis of aGVHD. In the CIV cohort, 21 (60%) patients had cGVHD; 12 (57.1%) of these patients were also diagnosed with aGVHD (P=.43). Most patients had multiple sites of cGVHD; however, there were no reports of liver site–associated cGVHD in either cohort.
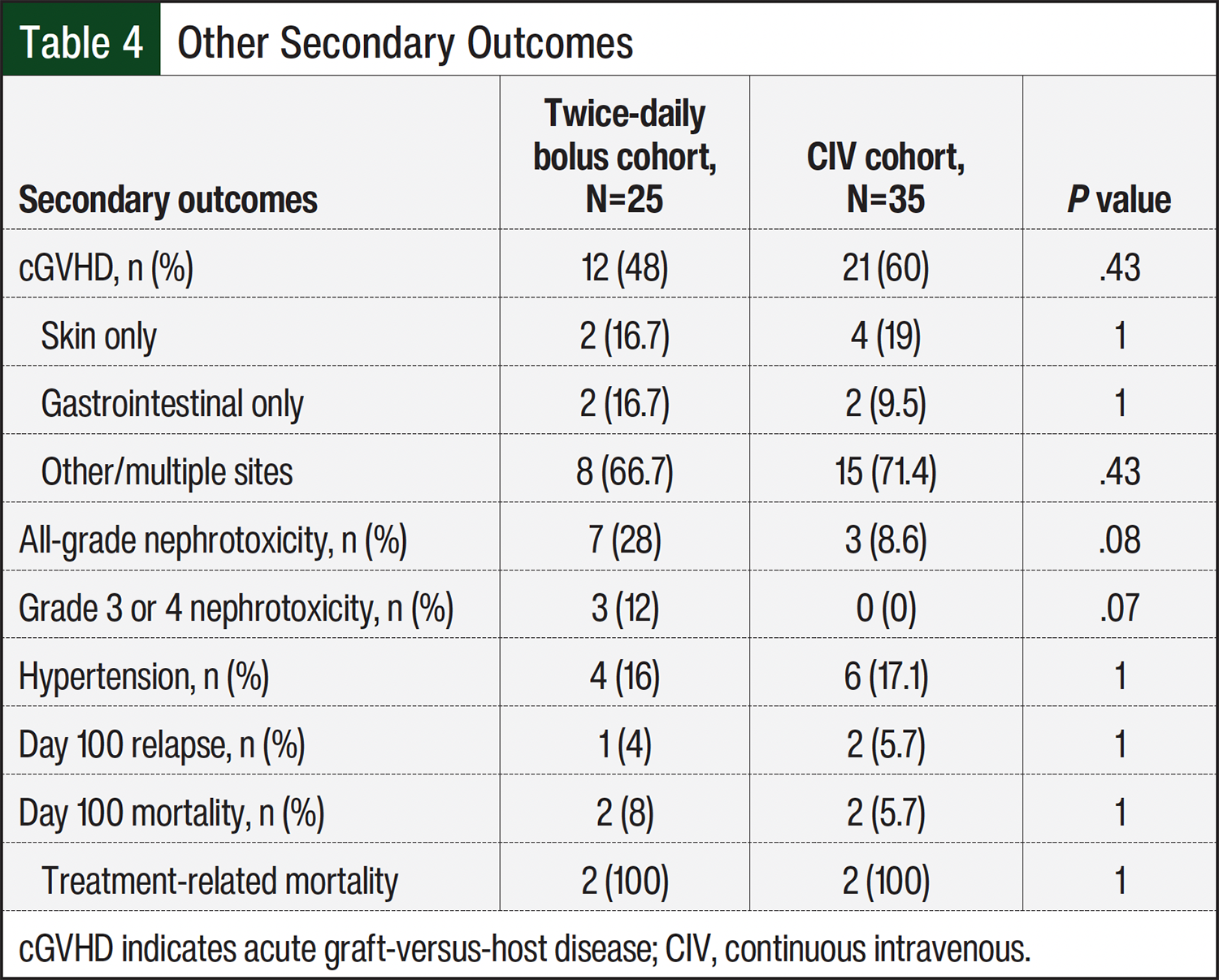
In all, 10 (16.7%) patients had nephrotoxicity while receiving tacrolimus. A total of 7 (28%) patients in the twice-daily bolus cohort and 3 (8.6%) patients in the CIV cohort had any-grade nephrotoxicity (P=.08; Table 4). In the twice-daily bolus cohort, 3 (12%) patients developed grade 3 or 4 nephrotoxicity compared with no patients in the CIV cohort. In all 3 patients, elevations in serum creatinine were transient and returned to baseline. Hypertension requiring pharmacologic intervention occurred in 4 (16%) patients in the twice-daily bolus cohort and in 6 (17.1%) patients in the CIV cohort (P=1).
One (4%) patient in the twice-daily bolus cohort and 2 (5.7%) patients in the CIV cohort had disease relapse by day 100 (P=1; Table 4). All-cause mortality by day 100 occurred in 2 patients from each cohort (P=1). Both patients in the twice-daily bolus cohort died from HSCT-related complications, including hepatic sinusoidal obstruction syndrome and intracranial hemorrhage after graft failure. Similarly, the causes of death for the 2 patients in the CIV cohort were also HSCT-related complications, including acute liver failure/septic shock and acute respiratory failure resulting from diffuse alveolar hemorrhage. There were no reports of relapse mortality by day 100.
Discussion
This is the first retrospective study to directly compare twice-daily bolus tacrolimus with CIV tacrolimus in adults who underwent allogeneic HSCT. Previous single-arm studies compared the rates of GVHD to historical controls.8,11 Our study’s rates of grade 2 to 4 aGVHD were comparable with the CIBMTR’s historical controls (44% for twice-daily bolus and 31.4% for CIV vs historical controls of 39%-59%).9 These rates are also consistent with other studies that evaluated twice-daily tacrolimus by Hashmi and colleagues (37%)8 and by Bacopoulos and colleagues (34.9%).11 These consistent aGVHD rates increase our study’s external validity and support the use of twice-daily bolus tacrolimus as an alternative to CIV tacrolimus.
It is important to consider shifts in the HSCT landscape that may have occurred over the study time frame when comparing these results to published literature. In recent years, the use of posttransplant cyclophosphamide-based immunosuppressant regimens has increased in HSCT recipients who are receiving grafts from mismatched or haploidentical donors. Recent studies have demonstrated that posttransplant cyclophosphamide decreases the incidence of GVHD compared with other standard regimens.15,16 In this study, posttransplant cyclophosphamide was used in combination with tacrolimus and mycophenolate mofetil in 43% of the entire population, notably in 100% of the haploidentical donor patients; more patients received posttransplant cyclophosphamide in the twice-daily bolus cohort. Furthermore, there was only 1 of 6 patients in the mismatched unrelated donors from the twice-daily bolus cohort who did not receive a posttransplant cyclophosphamide-based regimen. Conversely, there were no reports of posttransplant cyclophosphamide for aGVHD prophylaxis in Hashmi and colleagues’ study with tacrolimus plus mycophenolate mofetil and tacrolimus plus methotrexate.8 Bacopoulos and colleagues reported that the use of posttransplant cyclophosphamide was 2.9% of the population; however, this treatment was used in combination with cyclosporine and antithymocyte globulin for GVHD prophylaxis.11 Therefore, it is unknown how posttransplant cyclophosphamide may impact the rates of GVHD in the twice-daily bolus cohort versus the CIV cohort of this study.
The incidence of nephrotoxicity in this study was comparable to previous outcomes.8,11 It is standard practice at this institution to utilize oral tacrolimus for GVHD prophylaxis, with IV tacrolimus used only when there is a direct need (eg, an inability to swallow, absorption concerns). Most patients in this study required IV tacrolimus because of mucositis; with 2 patients having absorption issues with inconsistent oral tacrolimus levels. Increases in serum creatinine could be attributable to decreased oral intake in patients with mucositis, predisposing patients to acute kidney injury. Underlying renal dysfunction, such as chronic kidney disease, may also have contributed to these results.
Two patients in the twice-daily bolus cohort developed acute kidney injury that required transient dialysis; however, both cases were determined to be multifactorial. One of these patients had known stage IV chronic kidney disease at baseline. Both patients had decreased oral intake before switching from twice-daily bolus tacrolimus to IV tacrolimus, and both patients received concurrent nephrotoxic medications (eg, preparative chemotherapy, prophylactic anti-infective drugs). In addition, 2 patients who developed nephrotoxicity in the twice-daily bolus cohort also had tacrolimus levels of >15 ng/mL that resolved.
It is important to consider the potential differences in pharmacokinetic properties between twice-daily bolus and CIV administrations of tacrolimus. It is difficult to prove that the kinetics of bolus dosing led to supratherapeutic levels that resulted in nephrotoxicity, but this should be considered. Although there was not a direct correlation identified in this study, bolus administration may lead to a higher peak tacrolimus level, raising concerns about nephrotoxicity. Patients undergoing HSCT frequently require potentially nephrotoxic medications, such as antibiotics, loop diuretics, and acid suppression agents. There were no obvious medication confounders for renal dysfunction, but this issue could certainly play a role, and practitioners should be mindful. The rates of hypertension that require intervention were similar to the rates in previously published findings.8,11
Limitations
Because of its retrospective, single-center design, our study has limitations. As a result of initiating treatment for HSCT recipients with oral tacrolimus, there was a small sample size of IV tacrolimus recipients who may confound our results. Given its retrospective nature, our study’s end points depended on consistent provider documentation, which may lead to variability. Criteria for aGVHD diagnosis by day 100 may not have completely captured the patients who had aGVHD after this time frame. Furthermore, cGVHD, mortality, and disease relapse were assessed until the time of data collection, which increased the median follow-up time frame for only the CIV cohort.
Another consideration would be the heterogeneity of the donor type and the immunosuppressant regimens between the 2 cohorts. The twice-daily bolus cohort had a larger representation of mismatched unrelated donors, which may predispose HSCT recipients to a higher risk for GVHD. However, there was an increased utilization of posttransplant cyclophosphamide-based immunosuppression that may impact this risk.
This cohort study is applicable to current practice and captures relevant clinical outcomes to help guide decisions regarding the 2 methods of IV tacrolimus administration. Similar results of previously published tacrolimus administration studies suggest that twice-daily bolus administration may be an acceptable alternative. Although not formally assessed, there may be other advantages to twice-daily bolus administration, such as line accessibility and savings of tacrolimus vials through batch preparation as well.
Conclusion
Tacrolimus twice-daily bolus administration over 2 hours is comparable in efficacy and safety with CIV administration in adults who have undergone HSCT. Twice-daily bolus administration had similar rates of GVHD as CIV and historical controls. Patients receiving twice-daily bolus tacrolimus should be monitored closely for acute nephrotoxicity, especially in the setting of supratherapeutic levels or when multiple risk factors are present.
Author Disclosures
Dr Battiwalla has received research support from Autolus, BMS, Gilead Sciences, Johnson & Johnson, Kite Pharma, and Legend Biotech; is on the Advisory Board of and is a consultant to BMS, Incyte, Johnson & Johnson, Legend Biotech, and Sanofi; and is on the Speaker’s Bureau of Johnson & Johnson and Legend Biotech. Dr Wilson, Dr Parsons, Dr Abernathy, Dr Matthews, and Dr Siler have no conflicts of interest to report.
References
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Hematopoietic Cell Transplantation. Version 3.2025. September 24, 2025. Accessed March 3, 2026. www.nccn.org/professionals/physician_gls/pdf/hct.pdf
- Timofeeva OA, Philogene MC, Zhang QJ. Current donor selection strategies for allogeneic hematopoietic cell transplantation. Hum Immunol. 2022;83:674-686. doi:10.1016/j.humimm.2022.08.007
- Ramachandran V, Kolli SS, Strowd LC. Review of graft-versus-host disease. Dermatol Clin. 2019;37:569-582. doi:10.1016/j.det.2019.05.014
- Akahoshi Y, Spyrou N, Hogan WJ, et al. Incidence, clinical presentation, risk factors, outcomes, and biomarkers in de novo late acute GVHD. Blood Adv. 2023;7:4479-4491. doi:10.1182/bloodadvances.2023009885
- Prograf (tacrolimus) capsules, for oral use [prescribing information]. Astellas Pharma Inc; August 2023. Accessed February 12, 2026. www.accessdata.fda.gov/drugsatfda_docs/label/2023/050708s055,010115s007lbl.pdf
- Ratanatharathorn V, Nash RA, Przepiorka D, et al. Phase III study comparing methotrexate and tacrolimus (Prograf, FK506) with methotrexate and cyclosporine for graft-versus-host disease prophylaxis after HLA-identical sibling bone marrow transplantation. Blood. 1998;92:2303-2314.
- Nash RA, Antin JH, Karanes C, et al. Phase 3 study comparing methotrexate and tacrolimus with methotrexate and cyclosporine for prophylaxis of acute graft-versus-host disease after marrow transplantation from unrelated donors. Blood. 2000;96:2062-2068.
- Hashmi H, Bhandari S, Kumar R, et al. Twice-daily intravenous bolus tacrolimus infusion: a safe and effective regimen for graft-versus-host disease prophylaxis. Hematol Oncol Stem Cell Ther. 2020;13:232-237. doi:10.1016/j.hemonc.2020.03.002
- Jagasia M, Arora M, Flowers ME, et al. Risk factors for acute GVHD and survival after hematopoietic cell transplantation. Blood. 2012;119:296-307. doi:10.1182/blood-2011-06-364265
- Przepiorka D, Ippoliti C, Khouri I, et al. Tacrolimus and minidose methotrexate for prevention of acute graft-versus-host disease after matched unrelated donor marrow transplantation. Blood. 1996;88:4383-4389.
- Bacopoulos AJS, Ho L, Yang A, et al. Safety of two-hour intermittent intravenous infusions of tacrolimus in the allogeneic hematopoietic stem cell transplantation unit. J Oncol Pharm Pract. 2021;27:33-39. doi:10.1177/1078155220908948
- Harris AC, Young R, Devine S, et al. International, multicenter standardization of acute graft-versus-host disease clinical data collection: a report from the Mount Sinai Acute GVHD International Consortium. Biol Blood Marrow Transplant. 2016;22:4-10. doi:10.1016/j.bbmt.2015.09.001
- Jagasia MH, Greinix HT, Arora M, et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group Report. Biol Blood Marrow Transplant. 2015;21:389-401. doi:10.1016/j.bbmt.2014.12.001
- US Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE). Version 4.0. May 28,2009. Accessed March 1, 2023. https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/Archive/CTCAE_4.0_2009-05-29_QuickReference_8.5x11.pdf
- Moiseev IS, Pirogova OV, Alyanski AL, et al. Graft-versus-host disease prophylaxis in unrelated peripheral blood stem cell transplantation with post-transplantation cyclophosphamide, tacrolimus, and mycophenolate mofetil. Biol Blood Marrow Transplant. 2016;22:1037-1042. doi:10.1016/j.bbmt.2016.03.004
- Carnevale-Schianca F, Caravelli D, Gallo S, et al. Post-transplant cyclophosphamide and tacrolimus—mycophenolate mofetil combination governs GVHD and immunosuppression need, reducing late toxicities in allogeneic peripheral blood hematopoietic cell transplantation from HLA-matched donors. J Clin Med. 2021;10:1173. doi:10.3390/jcm10061173